Professional sports medicine has access to extraordinary resources. The best imaging available. Expert physiotherapists, surgeons, and rehabilitation specialists. Nutritional and biomechanical support at every level. And yet certain injuries in professional athletes follow a pattern that all of that infrastructure consistently fails to break: the chronic tendinopathy that does not resolve, the calf that keeps tightening, the elbow that stays painful through every treatment protocol tried.
The reason, in many of these cases, is that the injury is being treated at its endpoint while its actual driver in the cervical or thoracic spine goes unidentified.
What No Treatment for Tennis Elbow Actually Means
Tennis elbow, more precisely called lateral epicondylalgia, is one of the most common chronic pain presentations in both sports clinics and general pain practice. The Canadian Family Physician published a review examining the therapeutic effectiveness of every commonly used treatment for chronic tennis elbow, including corticosteroid injections, physiotherapy, massage, platelet-rich plasma, and stretching. Their conclusion was that no treatment for tennis elbow proved better than placebo long-term.
This finding is consistent with what systematic reviews of lateral epicondylalgia by Coombes and colleagues have repeatedly demonstrated: cortisone provides short-term relief but long-term outcomes remain poor, and most interventions perform similarly over time. A major randomized trial found that corticosteroid injection produced worse outcomes at one year than placebo. The literature increasingly characterizes tennis elbow as a degenerative tendinopathy rather than an inflammatory condition.
What the combined evidence actually establishes is that the average recovery from chronic tennis elbow is approximately two years, with or without treatment. The interventions we apply may provide temporary relief. They do not change the underlying recovery trajectory.
This is a striking finding for a condition that affects a large portion of the athletic population. If every local treatment fails similarly, a reasonable scientific question follows: is the tendon actually the origin of the problem?
The Cervical Spine Origin of Elbow Tendinopathy
The limbs evolved from the spine. The arms and upper limbs emerged developmentally from the cervical and upper thoracic spine. The nerve roots that supply motor and sensory function to the forearm and hand originate from C5 through T1. This anatomical relationship is the key to understanding why chronic tennis elbow so frequently has a cervical origin.
This connection is not unique to the neuromyofascial model. The regional interdependence model, widely accepted within sports physiotherapy, proposes that dysfunction in one region of the body contributes to pain and dysfunction elsewhere. Neck to elbow, hip to knee, lumbar spine to foot. The concept is now mainstream in sports medicine.
Mainstream clinical guidelines have begun to reflect this. The 2022 APTA/JOSPT clinical practice guideline for lateral elbow pain explicitly classifies a subgroup of patients as “Type 3: Elbow plus Cervical,” defined as lateral elbow symptoms combined with cervical signs and symptoms or neuropathic pain features. The same guideline lists cervical radiculopathy among the differential diagnoses that clinicians should actively consider when evaluating lateral elbow pain, and recommends that clinicians may use manipulation or mobilization directed at the cervical spine, thoracic spine, or wrist as an adjunct to local care when impairments in those regions are identified. This is not proof of cervical causation as the primary driver in every case, but it is guideline-level acknowledgment that refractory tennis elbow should not be evaluated as a tendon-only problem.
More specifically, research has demonstrated that C6 and C7 nerve root dysfunction can produce symptoms nearly identical to lateral epicondylalgia, and that cervical treatment improves elbow symptoms in selected patients with concurrent neck dysfunction. A 2023 study found radial nerve pressure-pain hypersensitivity and increased radial nerve cross-sectional area on the affected side in unilateral lateral epicondylalgia, supporting the idea that the radial nerve may be a peripheral driver of altered pain processing in some patients. A 2025 case-control study reported impaired cervical proprioception in people with lateral epicondylitis compared with asymptomatic controls.
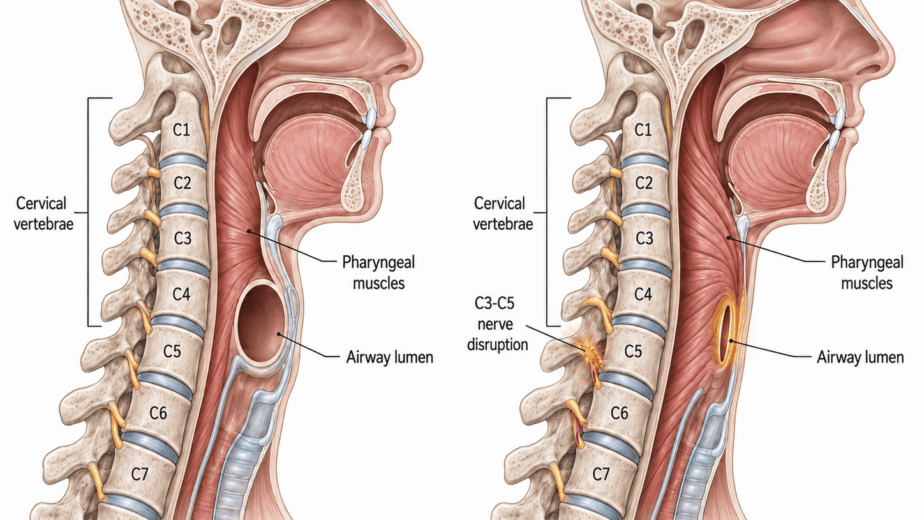
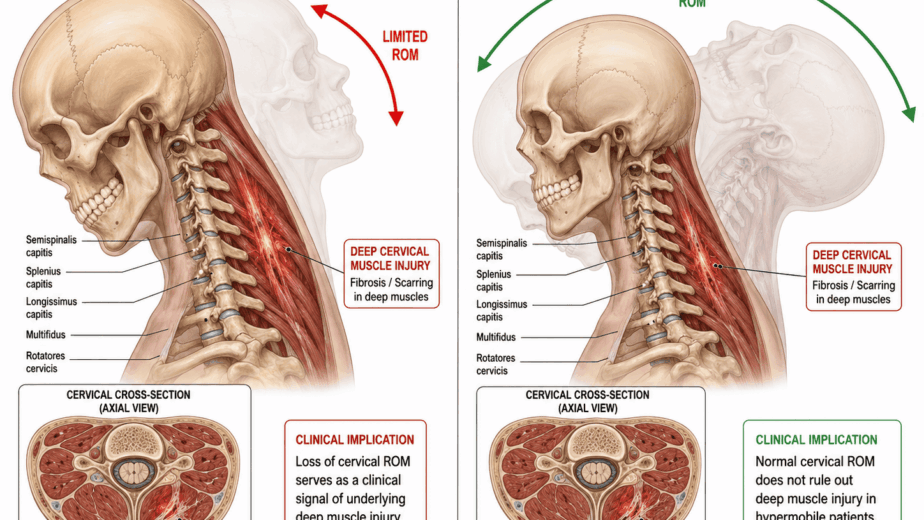
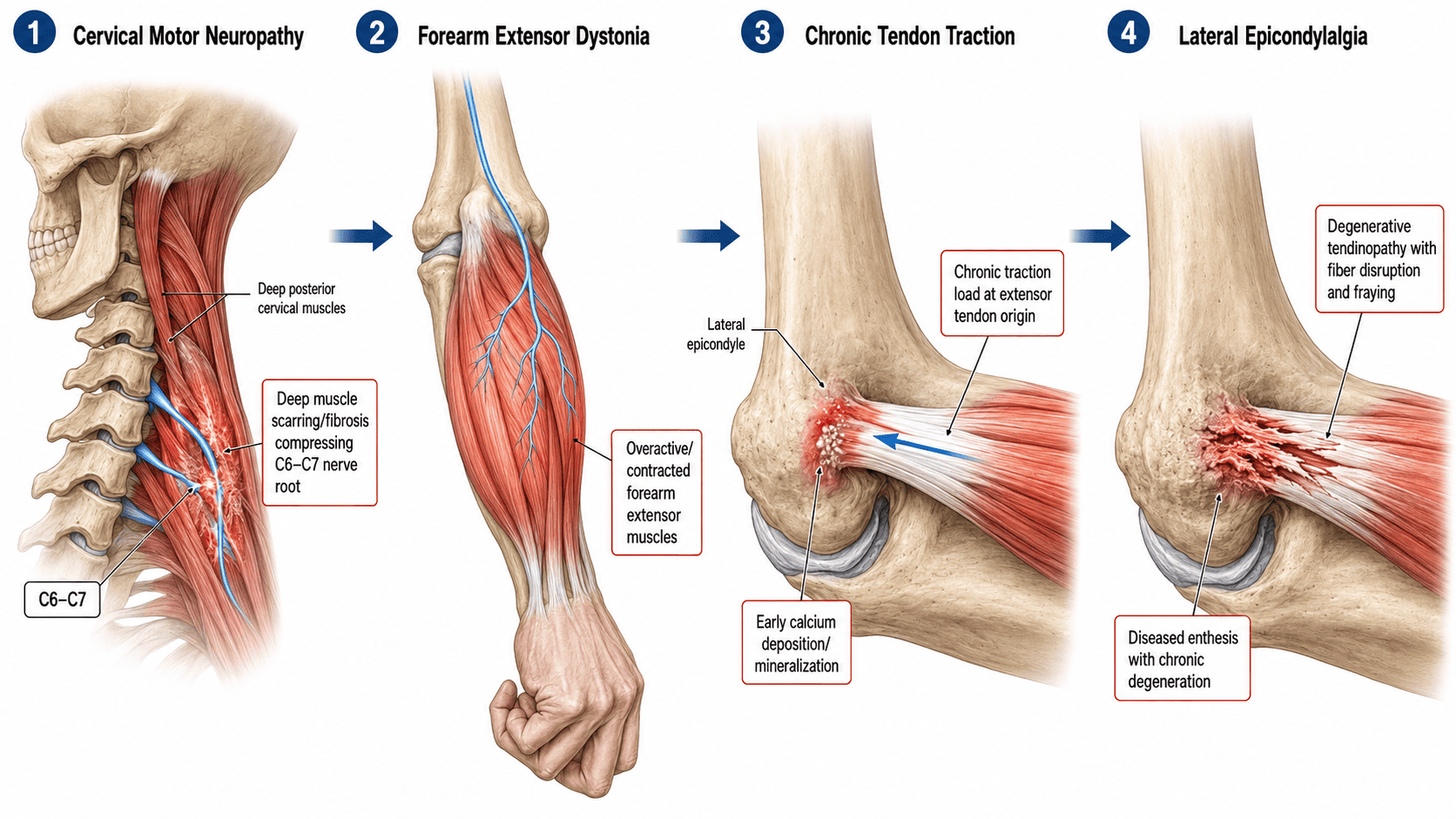
In the neuromyofascial model, the injury sequence in tennis elbow typically begins not at the elbow but in the cervical spine. Deep spinal muscle injury and scarring in the neck, often from a whiplash event, repetitive strain, or gradual accumulation of cervical pathology, creates persistent compression of the motor nerve roots supplying the forearm. That nerve root compression generates a motor neuropathy: impaired motor nerve signal reaching the forearm extensor muscles.
The effect of impaired motor nerve signal on muscle is dystonia. The motor end plate, the junction where the nerve connects to the muscle to deliver its signal, accumulates abnormal electrical activity when the nerve signal is disrupted. Rather than receiving a normal signal to relax and depolarize, the muscle enters a state of persistent involuntary shortening and spasm. The forearm extensor group, including the extensor carpi radialis brevis, becomes tonically contracted.
That sustained tonic contraction creates constant traction at the elbow. The tendon origin at the lateral epicondyle is under chronic load rather than normal intermittent load. This mechanism aligns directly with the Cook and Purdam continuum model of tendinopathy, which established that tendons deteriorate through excessive load, repetitive load, and poor load recovery rather than through acute inflammation. The neuromyofascial model proposes that in many refractory cases, the abnormal mechanical load originates in motor neuropathy at the cervical spine rather than in the elbow itself.
The body responds to the chronically stressed tendon by depositing calcium at the insertion. This calcification is associated with progressive tendon degeneration rather than representing a straightforward repair response. Over time, the combination of chronic dystonic tension, calcium deposition, and tendon microtrauma creates exactly the degenerative tendinopathy that standard imaging identifies at the elbow.
Treating the elbow directly addresses the endpoint of this sequence. The cervical motor neuropathy generating the forearm dystonia remains fully active. When the local treatment effect wears off, the same abnormal tension recreates the same elbow pathology.
This is a clinical hypothesis, not a proven universal mechanism. What is well established is that chronic lateral epicondylalgia in refractory cases shows consistent evidence of both peripheral and central pain sensitization beyond the tendon itself, that imaging findings correlate only weakly with symptom severity, and that the cervical spine is a documented contributor in a meaningful subgroup of patients. Clinical observations at the practice over approximately 30 years suggest that when the cervical and upper thoracic neuromyofascial pathology driving the forearm dystonia is identified and addressed, chronic tennis elbow presentations that have been resistant to every standard treatment frequently improve or resolve. These are clinical observations and do not constitute proof of causation.
Kevin Durant and the Achilles Tendon
In 2019, the Toronto Raptors made it to the NBA Finals against the Golden State Warriors. I live in the Greater Toronto Area and, like most Canadians, was following the series closely.
Before Game 5, I was out with a small group of physicians and businesspeople in Toronto. We were discussing the series and the question of whether Kevin Durant would return to play despite having been sidelined for weeks with calf pain. The medical staff around him were publicly confident he would be able to play.
I want to be clear that I have never treated Kevin Durant and have no knowledge of the details of his private medical care beyond what was publicly reported.
What I said to that group was that I did not believe his calf pain had ever been properly investigated for its underlying cause, and that I did not think he would make it through the game. My reasoning was that the public reporting suggested his care had focused on the calf and Achilles tendon locally, and that there was no indication the motor neuropathy that, in my clinical experience, can underlie chronic Achilles tendinopathy and calf dysfunction in refractory cases had been identified or treated.
The sports medicine literature supports the upstream logic in principle. Research consistently finds that prior calf dysfunction increases risk for Achilles tendinopathy and Achilles rupture. And S1 nerve root dysfunction, one of the most common lumbar radiculopathy presentations, frequently creates calf weakness, altered gait, and reduced push-off strength. The pathway from lumbar nerve root compromise to calf dysfunction to Achilles vulnerability is anatomically and clinically plausible.
It is worth being precise here. The Achilles literature differs from the tennis elbow literature in one important respect: loading-based rehabilitation does demonstrate meaningful benefit for Achilles tendinopathy across multiple systematic reviews, and current clinical guidelines recommend tendon-loading exercise as effective first-line care. The failure of local treatment that characterizes refractory tennis elbow is not as clearly established for Achilles presentations generally. The neuromyofascial argument for Achilles cases is strongest in the refractory patient: the one who has completed appropriate loading rehabilitation, whose symptoms persist or keep returning, and whose proximal kinetic chain and lumbar nerve root contribution have never been systematically investigated.
In those cases, the same mechanism I described for tennis elbow applies through the lumbar and sacral nerve roots supplying the calf. Motor neuropathy at L5 or S1 creates dystonia in the gastrocnemius and soleus. The sustained tonic contraction of the calf places the Achilles tendon under chronic abnormal load. Over time the tendon develops degenerative changes: altered collagen organization, increased type III collagen deposition, and microtears at the insertion. In my clinical view, this progressive process is the underlying driver in a meaningful subset of recurrent and refractory Achilles presentations, not an acute isolated event.
Durant ruptured his Achilles in the first half of Game 5. He did not return to play for 552 days. Whether his prior calf symptoms reflected a lumbar neural component, incomplete local healing, altered loading mechanics, or something else entirely cannot be determined from public information alone. The case illustrates the clinical reasoning rather than proving the mechanism.
The Broader Athletic Picture
The most common chronic injuries in professional basketball, plantar fasciitis, Achilles tendinopathy, patellofemoral syndrome, hip-spine syndrome, and lower back pain, all involve tendons or joints under abnormal chronic load. In refractory cases where standard local rehabilitation has been completed appropriately and symptoms persist, the source of that abnormal load frequently warrants investigation beyond the symptomatic site.
Athletes who are screened and assessed for neuromyofascial pathology before injury develops, rather than after, have an opportunity to address spinal motor neuropathy before it produces the tendon degeneration and eventual rupture that ends seasons and careers.
The performance implication is equally significant. A motor neuropathy does not only create pain. It reduces the quality and output of the motor signal reaching the muscles it supplies. Research consistently demonstrates that nerve root irritation leads to reduced motor unit recruitment, altered firing patterns, muscle weakness, and impaired coordination. Maximizing neurological integrity from the spine outward to the limbs means more complete and coordinated motor recruitment, which translates directly into power output, speed, and injury resilience.
The strongest evidence-based version of this argument is straightforward: do not stop at the tendon in chronic refractory cases. The spine, the neural pathways, and the full kinetic chain deserve systematic investigation when local treatment has reached its ceiling. That position is now reflected in mainstream clinical guidelines. The neuromyofascial framework takes it further, proposing that spinal motor neuropathy is the primary upstream driver in many of these cases. That stronger claim remains a clinical hypothesis requiring prospective investigation. The clinical results, however, are consistent with it.
The information in this article is educational and informational in nature. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. If you are experiencing chronic tendinopathy or recurring athletic injury that has not responded to standard treatment, consult with a qualified healthcare provider to discuss the options appropriate for your situation.