Most of what I know about chronic spinal pain, I first learned from my own body.
In 1992, I sustained complex spinal injuries from a diving accident. The impact was catastrophic. I was a physician, and I went looking for the best available care. What I found was a system that was very good at identifying what was structurally wrong but far less equipped to address why recovery stalled or what to do when standard rehabilitation reached its limit.
Over several years, I recovered fully. But the process of getting there required me to develop approaches that did not yet exist in any coherent clinical framework. That experience became the foundation of everything I have built since.
The Problem I Kept Seeing
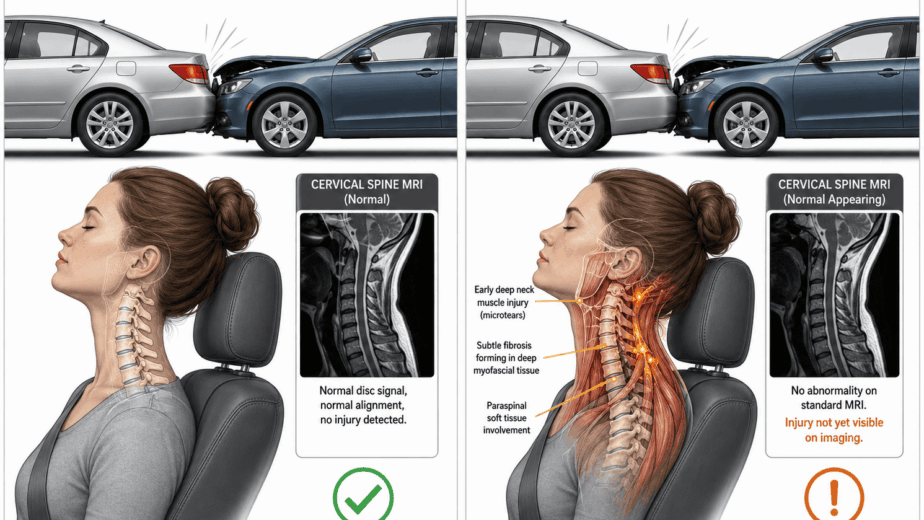
The patients who came to me were not unusual. Many had been in accidents, sustained sports injuries, or accumulated damage over years of demanding physical work. They had been through imaging, physiotherapy, specialist referrals. Many had been told their imaging was normal or that there was nothing more to offer.
Their pain was real. The problem was that medicine was looking for it in the wrong places, or with the wrong tools, or stopping the investigation too early.
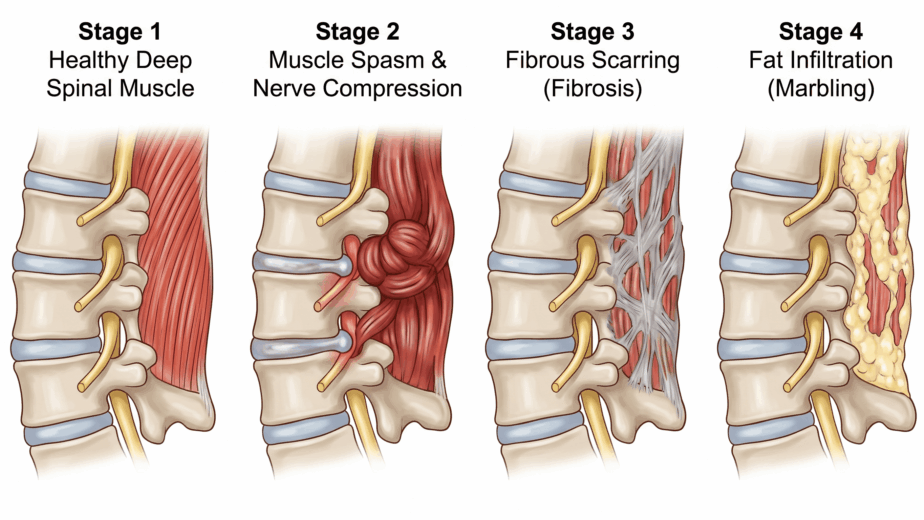
What I observed over years of clinical work was a consistent pattern: chronic pain was not a condition that lived in isolation in one tissue or one joint. It was the downstream result of accumulated neuromyofascial injury across multiple sites. And those sites could be identified, mapped, and addressed in a way that symptom management alone could not achieve.
This is the central premise of Neuromyofascial Science. Not that pain is imaginary when imaging is normal. Not that patients need to manage and adapt. But that the specific structural drivers of persistent symptoms can often be found when you know what to look for and how to look for it.
What the Framework Investigates
A diagnostic label tells you what a patient is experiencing. Neuromyofascial Science asks what is generating the experience.
For any given patient, that question requires building a map: a reconstruction of their injury history, the tissues involved, the neural pathways under load, the sites where fibrosis and scarring have altered normal anatomy and mechanics. The map is specific to the individual. Two patients with the same diagnosis may have entirely different underlying injury patterns, which is one reason why standard protocols produce such variable results.
The investigation follows a simple but important logic. Symptoms are treated as information. Where pain refers, how it behaves with movement, what other symptoms accompany it, when it started and how it has evolved: all of this points toward specific anatomy. The goal is to work backward from symptoms to the injury sites driving them.
This is what I mean by reverse engineering chronic pain.
Building the Clinical Tools
The investigational framework needed clinical tools to match it. Over thirty years and more than 80,000 hours of research and patient care, I developed and refined a range of targeted interventions designed to address neuromyofascial pathology directly rather than managing symptoms at the surface.
In 2002, I developed a spinal Botulinum toxin program, which was patented. This approach delivers neuromodulatory agents into specific spinal regions to create sustained chemical decompression, supporting non-surgical recovery of spinal components in cases involving disc herniation, spinal arthritis, and spinal stenosis.
Since then, the clinical toolkit has expanded significantly. The range of conditions addressed through Neuromyofascial Science now includes spinal concussion syndrome, spinal myelopathic syndrome, migraine, tinnitus, vertigo, fibromyalgia, frozen shoulder, cervical dystonia, complex arthritic presentations, and a number of other chronic and post-injury conditions where standard care has not produced recovery.
These are not separate treatment programs applied generically. They are precision interventions deployed based on the specific injury map of the individual patient.
What This Means for Patients
The patients I see have often already been through the standard pathway. They have not failed medicine. Medicine has not yet had the right tools to fully investigate their injury pattern.
Neuromyofascial Science does not position itself against standard care. Appropriate medical workup, imaging, neurology, and specialist assessment are all part of a complete picture. What NMFS adds is a more granular investigational layer: one focused on identifying the specific neuromyofascial pathology that may be driving persistent symptoms when standard findings appear normal or when standard treatment has reached a ceiling.
The question I have always come back to is a straightforward one. When a patient is still in pain after every standard option has been tried, is it more likely that nothing is wrong or that the right question has not yet been asked?
Thirty years of clinical work have given me a consistent answer.
The information in this article is educational and informational in nature. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. If you are experiencing chronic pain, consult with a qualified healthcare provider to discuss the options appropriate for your situation.