
CONDITIONS
TMJ & Tinnitus
Tinnitus and temporomandibular joint dysfunction are almost always treated as separate conditions, one sent to an audiologist, the other to a dentist. NMF Science investigates whether both are actually downstream symptoms of a single underlying injury pattern originating in the cervical and upper thoracic spine. When the spine is mapped as the source rather than the ear or the jaw, the clinical picture changes significantly, and so does the path toward lasting relief.
Current Medical Understanding
Tinnitus is typically understood as a hearing problem originating in the inner ear. The persistent ringing, humming, or hissing that characterizes tinnitus is most often attributed to damage of the delicate hair cells inside the cochlea, or to dysfunction of the auditory nerve. Treatment focuses on managing the sound perception through hearing aids, sound therapy, and in some cases medication. There is no widely accepted cure.
Temporomandibular joint disorder, or TMJ dysfunction, is understood as a problem with the jaw joint itself. The clicking, locking, and pain associated with TMJ are attributed to joint misalignment, stress-related clenching, or dental occlusion problems. Treatment focuses on the joint and surrounding muscles through bite guards, dental work, physical therapy, and occasionally surgical intervention on the joint.
The clinical challenge is that these two conditions rarely appear in isolation. People with tinnitus frequently also report neck pain, headaches, and jaw discomfort. People with TMJ dysfunction show similar symptom clustering. Systematic reviews show that people with TMJ disorder are approximately four times more likely to also have tinnitus, and studies indicate that up to 53 percent of people develop tinnitus following a concussion. Yet the standard medical approach continues to route patients to separate specialists who treat each symptom as an isolated local problem. The connection between them remains largely unaddressed.
NMF Science Perspective
NMF Science does not replace audiological or dental care for tinnitus and TMJ dysfunction. What it does is investigate whether both conditions share a common structural origin in the cervical and upper thoracic spine, and whether mapping that origin produces a more complete and actionable picture of what is driving the symptoms.
The mechanism begins with trauma. Acceleration-deceleration events such as whiplash from a motor vehicle collision, or years of cumulative biomechanical strain, cause microscopic tearing across the cervical and thoracic vertebrae. The body responds by forming dense neuromyofascial scar tissue around the injured area. Over time this tissue becomes pathological, restricting normal spinal movement and initiating a cascade of effects that reach all the way into the jaw and inner ear through two specific neurological pathways.
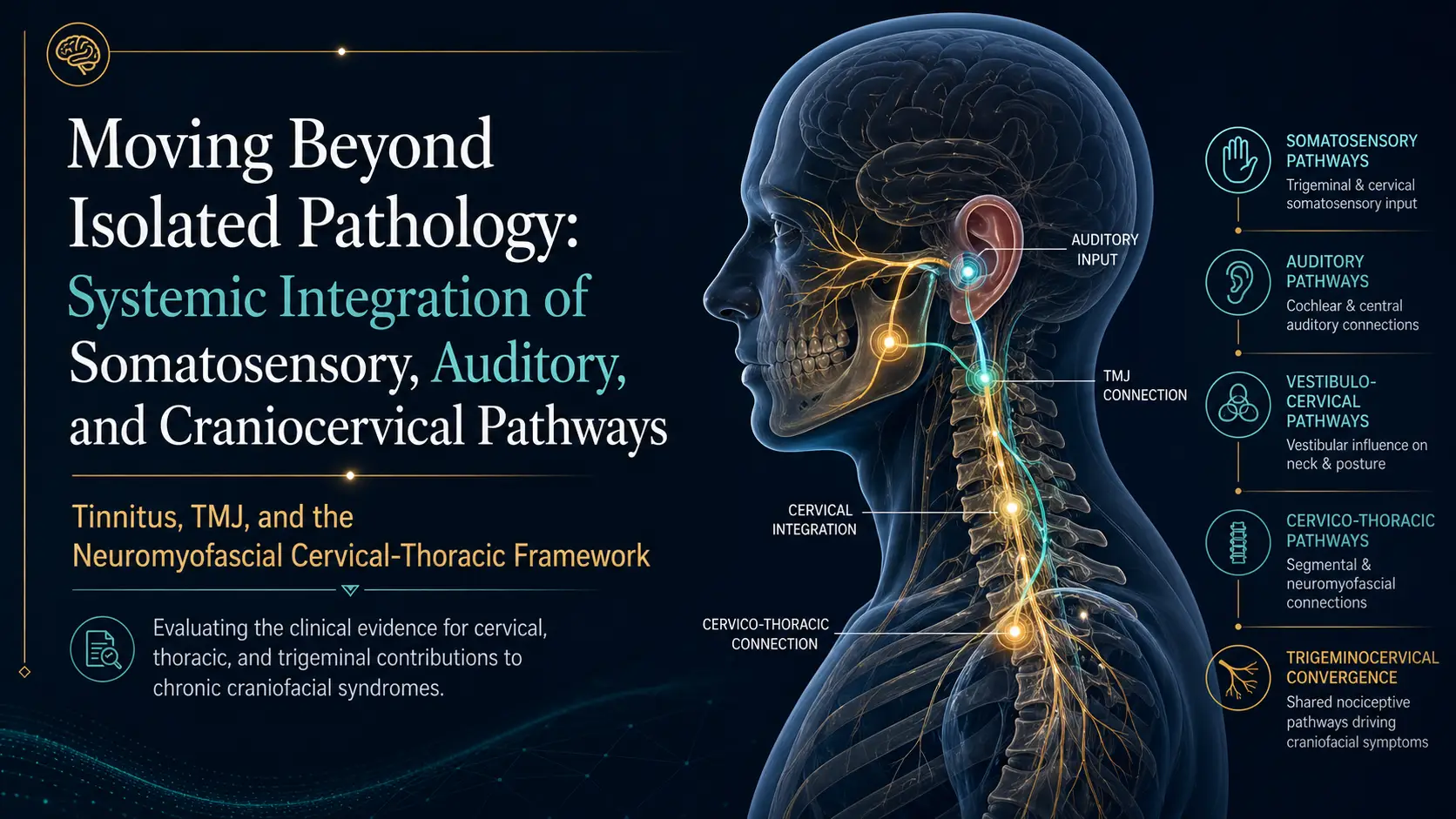
The first pathway runs through the trigeminal cervical complex, or TCC. This is the brainstem junction where signals from the trigeminal nerve, which serves the face, jaw, and chewing muscles, converge with signals from the cervical nerves serving the neck. Chronic cervical spine strain prompts the release of inflammatory neuropeptides at this junction, dramatically lowering the pain threshold throughout the craniofacial network. This is why a flare-up of cervical spine tension can produce stabbing pain behind the eyes, jaw locking, or severe headache. The jaw is not the source. It is the endpoint of a mechanical chain beginning in the spine.
The second pathway runs through the dorsal cochlear nucleus, or DCN. Adjacent to the TCC, the DCN is the primary auditory relay station where sound signals from the ear meet sensory signals from the neck and jaw. When this hub is overwhelmed by injury signals from the cervical spine, the brain misinterprets physical tension as auditory noise. The result is somatosensory tinnitus. The ringing is not coming from the ear. It is the brain's misreading of mechanical tension data as sound. This mechanism is confirmed by a straightforward clinical observation: in patients with somatosensory tinnitus, clenching the jaw, turning the head, or pressing on specific muscles in the neck changes the pitch or volume of the ringing in real time.
Both conditions also connect through OCT findings. Optical coherence tomography measures the microscopic thickness of the retinal nerve fiber layer, which is an extension of the central nervous system. Research documents retinal thinning in patients with chronic migraines, traumatic brain injury, and MS. Emerging evidence suggests similar thinning in patients with chronic tinnitus and TMJ dysfunction. The proposed mechanism is that persistent spinal cord tethering creates indirect mechanical stress along the neurological chain from the spine through the brainstem and into the optic nerve and retina. This is presented as a hypothesis and an active area of research, not settled clinical fact.
This does not mean tinnitus originates exclusively in the spine in every patient, nor that all TMJ dysfunction is caused by cervical pathology. It means that in a meaningful subset of patients, a treatable spinal injury pattern may be driving or amplifying both conditions simultaneously. Mapping that pattern is the starting point for understanding the full picture.
When the Ear and Jaw Are Blamed for a Spinal Problem
One of the most consistent patterns observed in patients presenting with both tinnitus and TMJ dysfunction is the presence of cervical spine trauma in their history, often from an event that occurred years before the ear and jaw symptoms became chronic. A rear-end collision, a sports impact, or prolonged postural strain gradually builds the neuromyofascial injury pattern that eventually overloads the TCC and DCN. By the time the tinnitus and jaw pain become severe enough to seek specialist care, the cervical origin has been long forgotten or never connected to the symptoms at all.
The jaw dysfunction component follows a specific pattern worth understanding clearly. Cervical spine injury triggers dystonia in the mastication muscles, including the temporalis, masseter, and pterygoid muscles. Dystonia here means a state of chronic involuntary spasm. These powerful chewing muscles, locked in constant low-grade spasm, pull the jaw off its natural hinge. This produces the clicking, locking, and pain of TMJ dysfunction as a secondary mechanical consequence of muscles overcompensating for structural damage deeper in the cervical spine. The joint itself is the endpoint, not the origin.
The broader significance of this pattern is that tinnitus and TMJ dysfunction are frequently early indicators of a larger neuromyofascial injury spectrum. Clinical observations consistently show that patients presenting with both conditions also carry overlapping diagnoses of post-concussion syndrome, migraine, fibromyalgia, and in some cases MS-spectrum presentations. Rather than representing five separate conditions, these may represent different expressions of one underlying spinal injury pattern at different stages of progression. The neuromyofascial map is the tool that connects these dots and makes targeted investigation possible.
What We Investigate
→ History of acceleration-deceleration trauma, concussive events, sports impacts, or cumulative postural strain that may have initiated the cervical injury pattern driving craniofacial and auditory symptoms.
→ Craniocervical junction integrity at C0-C1 and C1-C2 as a primary structural driver of trigeminal nerve irritation, jaw muscle dystonia, and auditory pathway disruption.
→ Somatosensory tinnitus confirmation: whether jaw clenching, head rotation, or cervical muscle pressure changes the pitch or volume of tinnitus, indicating DCN involvement rather than isolated cochlear damage.
→ Trigeminal cervical complex involvement: whether craniofacial pain, jaw locking, eye pain, or headache distribution maps to TCC-mediated referral patterns from cervical nerve irritation.
→ Dystonia in the mastication muscles including the temporalis, masseter, and pterygoid, and whether this represents primary TMJ pathology or secondary spasm from cervical spine injury.
→ Cervical and upper thoracic range of motion, segmental restriction, vertebral alignment, and fibrosis patterns at key injury sites that may not be visible on standard MRI.
→ Hypermobility as a diagnostic blind spot: whether normal or excessive cervical range of motion is masking deeper structural injury and neuromyofascial scarring at the craniocervical junction.
→ OCT findings: whether retinal nerve fiber layer thinning is present, and whether this correlates with the broader cervical and craniofacial injury pattern rather than representing isolated auditory or ophthalmic pathology.
→ Overlapping condition pattern: whether the patient also carries diagnoses of post-concussion syndrome, migraine, fibromyalgia, or other conditions suggesting a shared neuromyofascial spectrum driving multiple symptom clusters simultaneously.
→ Treatment response as a mapping tool: whether targeted neuromyofascial intervention at cervical injury sites produces measurable change in tinnitus pitch or volume, jaw mobility, or craniofacial pain, confirming the spinal origin of the symptom pattern.
Learn More About TMJ and Tinnitus
Below you will find our most comprehensive educational resources on TMJ dysfunction and tinnitus from the NMF Science perspective. Explore detailed video explanations, clinical slideshows, podcasts, and in-depth articles examining the cervical and neuromyofascial contribution to these two frequently misconnected conditions.
Videos
Slideshows
Social Media Videos
