CONDITIONS
Sciatica and Lower Limb Radiculopathy
Sciatica is typically explained as a single herniated disc compressing a nerve root at the lower lumbar spine. Yet patients with nearly identical MRI findings experience wildly different levels of pain and disability. Some have mild intermittent discomfort. Others develop severe leg weakness, sudden instability, or pain radiating in patterns that do not match the expected nerve distribution at all. NMF Science investigates why that variability exists and what the neuromyofascial map reveals about the broader mechanical failure that standard disc-focused care is not designed to fully address.
Current Medical Understanding
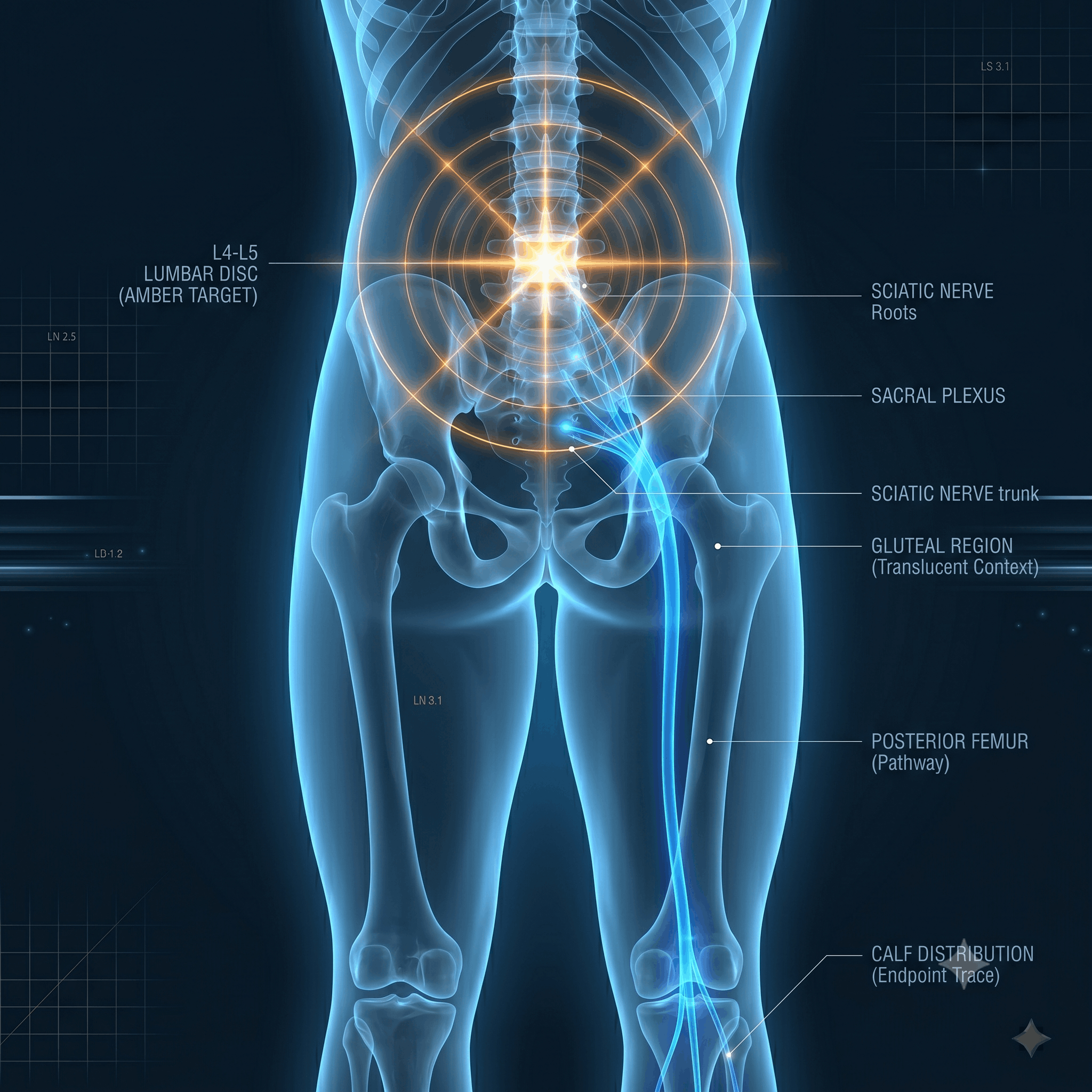
Sciatica is traditionally described as pain caused by compression of the sciatic nerve or its roots at the lower lumbar spine, most commonly at the L4-L5 or L5-S1 level. A herniated or bulging disc is the most frequently cited cause. Diagnosis relies on symptom patterns and imaging through MRI or CT scans. Conventional treatment targets the compression directly through rest, anti-inflammatory medications, physical therapy, epidural steroid injections, and in some cases surgical decompression.
Many patients improve with this approach, particularly in acute presentations where the disc herniation is the primary driver. The clinical challenge arises in chronic and recurrent cases. Many patients improve only partially or find that symptoms return after a period of relief. The significant variability in pain and disability between patients with similar imaging findings suggests that disc compression alone does not fully explain the spectrum of sciatica presentations.
Spinal stenosis, a narrowing of the spinal canal, is also commonly identified as a driver of sciatic-type symptoms. Standard medicine treats it as a structural narrowing at one or two spinal levels. What is less often considered is whether the stenosis represents the endpoint of a broader mechanical breakdown rather than a single anatomical problem requiring a single anatomical solution.
NMF Science Perspective
NMF Science does not dismiss the role of disc herniation or spinal stenosis in sciatica. What it investigates is the broader mechanical failure that creates and sustains nerve root compression, and why standard treatment often produces incomplete or temporary relief when that broader failure remains unaddressed.
The NMF Science framework proposes that chronic sciatica typically stems from accumulated injuries that have created neuromyofascial pathology around the paraspinal muscles of the lumbar spine. Scar tissue and fibrosis in these muscles alter the normal anatomy and mechanics of the lower back. The most significant consequence is a loss of normal lumbar lordosis, the natural inward curve of the lower spine. When that curve straightens, the vertebrae no longer articulate smoothly, internal disc pressures shift, and nerve roots exiting the spine experience persistent mechanical tension rather than simple point compression.
This mechanical tension acts as a tethering force. Rather than a single pinch point, the nerve root is subject to sustained pulling as it exits the spine and travels down the leg. A 2023 meta-analysis by Lin confirmed that neural mobilization techniques focused on restoring mechanical movement to tethered nerve tissue effectively reduce radicular pain, supporting the clinical significance of nerve tethering as a driver of sciatica beyond local disc compression alone.
Motor neuropathy from chronic nerve root irritation drives additional downstream consequences. Muscle dystonia, spasticity, and trigger point formation develop in the pelvis, hip, thigh, calf, and foot as secondary responses to the compromised nerve supply. These downstream changes amplify pain and disability significantly beyond what the spinal compression alone would produce. The combination of spinal tethering above and motor neuropathy below is what creates the full spectrum of sciatic disability.
Spinal stenosis in this framework is not a single-level narrowing. Clinical observations and imaging confirm that severe stenosis results from multiple areas of vertebral misalignment creating what might be described as a jagged pathway through the spinal canal. Normal nerve gliding is replaced by multipoint tethering and erratic vertebral movement. This distributed mechanical failure cannot be resolved by addressing a single disc level. It requires evaluating and treating the lumbar spine, lower thoracic spine, pelvis, hips, and lower limbs as a single unified structural and neuromyofascial system.
This does not mean that surgical decompression is never appropriate or that imaging findings are irrelevant. It means that in cases of chronic, complex, or treatment-resistant sciatica, the neuromyofascial map of the full lower limb system deserves investigation alongside the structural findings that standard imaging captures.
When Sciatica Does Not Follow the Expected Pattern
One of the most diagnostically important patterns in complex sciatica is the atypical presentation. Classic sciatica follows a predictable nerve root distribution. L4 produces lateral thigh and shin pain. L5 produces outer calf and top-of-foot symptoms. S1 produces posterior calf and heel symptoms. When a patient's pain does not follow these distributions, or when multiple distributions are involved simultaneously, standard care often struggles to find a satisfying explanation.
NMF Science identifies these atypical presentations as valuable diagnostic clues. Pain along the outer thigh and calf without foot numbness, an externally rotated gait pattern, sudden leg heaviness or legs that give way on stairs, or pain concentrated in the hip and upper lower back rather than the classic sciatica distribution, all point toward concurrent injuries involving both the thoracic and lumbar spine rather than a single disc level. This is what clinical literature describes as hip-spine syndrome, where overlapping pathologies from adjacent spinal regions create a complex picture that neither hip nor spine investigation alone fully explains.
Coordination loss and clumsiness are also commonly reported in these complex presentations. When chronic nerve root irritation produces measurable motor unit loss and remodeling in the leg muscles, the neurological signals governing precise movement become compromised. The result is not just pain but altered motor control that affects gait, balance, and the ability to navigate stairs or uneven surfaces safely. Mapping the full neuromyofascial system from the thoracic spine through the pelvis and down to the foot is what identifies which components of this complex picture are contributing to each specific symptom.
What We Investigate
→ Severity and location of nerve root compression at L4-L5 and L5-S1 and whether the structural cause is disc herniation, fibrosis, loss of lordosis, or a combination of factors at multiple levels.
→ Loss of normal lumbar lordosis and whether straightening of the lumbar curve is creating persistent mechanical tethering of the nerve root beyond the local compression that imaging identifies.
→ Paraspinal fibrosis patterns around the lumbar segments and whether scar tissue from old injuries is destabilizing spinal mechanics and driving the conditions that sustain nerve root irritation.
→ Motor neuropathy in the leg: whether calf muscles, hip stabilizers, gluteal muscles, or foot intrinsic muscles show signs of dystonia, weakness, spasticity, or trigger point formation consistent with chronic nerve root involvement.
→ Sensory neuropathy patterns: whether pain, numbness, tingling, or coordination loss follows specific nerve root distributions or spans multiple distributions suggesting multi-level involvement.
→ Atypical presentations including outer thigh pain without foot symptoms, externally rotated gait, leg heaviness, sudden give-way episodes, or hip-dominant pain suggesting hip-spine syndrome rather than single-level disc compression.
→ Lower thoracic spine involvement and whether concurrent thoracic injury is contributing to the lower limb neuropathy picture in ways that lumbar-only assessment would miss.
→ Dynamic mechanical issues that static MRI may not capture: movement-dependent stenosis, load-bearing effects on the spinal canal, or postural changes that reveal tethering not visible in a resting scan position.
→ Trigger point formation in pelvic, gluteal, hamstring, calf, and foot muscles that are amplifying radicular pain beyond the level of spinal compression alone and sustaining the disability cycle.
→ Treatment response patterns: whether neural mobilization, lumbar neuromyofascial intervention, or pelvic and hip rehabilitation produce measurable improvement in leg symptoms, confirming the mechanical and neuromyofascial contribution to the overall symptom map.
Learn More About Sciatica
Below you will find our most comprehensive educational resources on sciatica and lower limb radiculopathy from the NMF Science perspective. Explore detailed video explanations, clinical slideshows, and in-depth articles examining the full mechanical picture behind sciatic nerve pain, the hip-spine syndrome concept, and what neuromyofascial mapping adds to our understanding of why some sciatica presentations resist standard treatment.
Videos
Slideshows