CONDITIONS
Elbow Pain
Elbow pain labeled as tennis elbow or lateral epicondylalgia is one of the most commonly treated yet persistently misunderstood musculoskeletal conditions. Standard care focuses on the tendon as the source of the problem. NMF Science investigates whether the cervical and upper thoracic spine may be the upstream driver, producing motor neuropathy that continuously loads the tendon from the inside out through abnormal muscle activity. When that spinal driver is mapped and addressed, the picture of why local-only treatment so often falls short becomes much clearer.

Current Medical Understanding
Tennis elbow, more accurately described as lateral epicondylalgia, is characterized by pain over the lateral epicondyle of the humerus and tenderness at the origin of the wrist extensor tendons. The extensor carpi radialis brevis is the most commonly involved structure. Symptoms include pain with gripping or resisted wrist extension, perceived tightness, and forearm weakness. Repetitive strain and overuse are the most commonly cited causes.
Standard treatment focuses on the local area. Rest, anti-inflammatory medications, corticosteroid injections, forearm strengthening exercises, physiotherapy, platelet-rich plasma injections, and in some cases surgical release of the tendon are the primary options. Each of these approaches treats the tendon as the origin of the problem.
The clinical challenge is that chronic lateral epicondylalgia can persist for months or years despite these interventions. Systematic reviews of treatment outcomes show variable and often modest benefit, particularly in long-term follow-up. Many patients improve partially but see symptoms return. When compared to other soft tissue injuries of far greater complexity that resolve predictably within known healing timelines, the prolonged and unpredictable recovery pattern of some chronic elbow pain cases raises an important question: is there an upstream driver contributing to persistence that local treatment is simply not reaching?
NMF Science Perspective
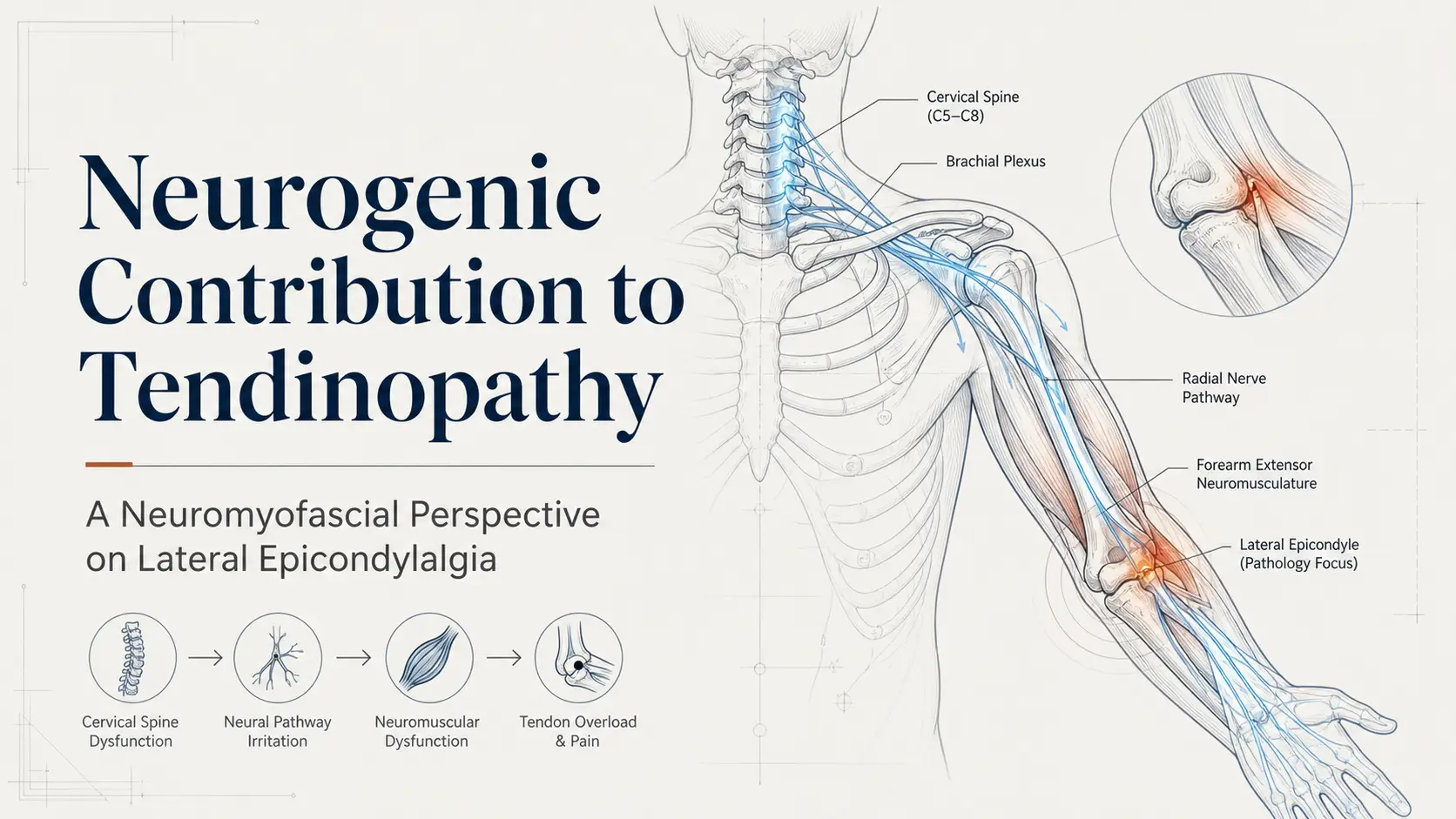
NMF Science does not dismiss the local tendon pathology in lateral epicondylalgia. What it investigates is whether motor neuropathy originating in the cervical and upper thoracic spine may be the upstream driver creating the persistent muscle dysfunction that continuously loads the tendon from above.
The proposed mechanism chain is specific. Injury or dysfunction in the cervical spine and cervicothoracic junction produces paraspinal myofibrosis. That myofibrosis alters motor nerve signaling along the radial nerve distribution serving the forearm extensor muscles. The result is a persistent low-grade dystonia in subsets of the forearm extensor muscle fibers. Those dystonic fibers maintain sustained hypertonicity, generating abnormal and continuous traction at the common extensor tendon origin on the lateral epicondyle. Over time this abnormal traction increases tensile load, contributes to microtrauma, impairs normal tendon remodeling, and promotes degenerative tendinopathy rather than the acute inflammation that standard treatment is designed to address.
This framework reframes lateral epicondylalgia from a purely local tendon disorder to a systems-based neuromuscular condition involving spinal motor control, fascial integrity, and distal biomechanical loading. The tendon is not the source. It is the endpoint of a mechanical chain beginning in the spine.
Clinical observations from Dr. Lamb's practice over approximately 30 years suggest that chronic tennis elbow is frequently associated with neuromyofascial dysfunction at the cervical spine segments, the cervicothoracic junction, and the upper thoracic paraspinal tissues. In more complex presentations including repetitive strain injury and chronic regional pain syndrome, multiple levels of cervical and thoracic neuromyofascial dysfunction are often observed on the affected side. Some published literature also suggests that cervical spine-directed therapy may improve outcomes in chronic lateral elbow pain, supporting investigation of proximal contributors alongside local treatment.
This does not mean local tendon pathology is not real or that standard treatment is without value. It means that in cases of chronic, treatment-resistant elbow pain, the cervical and upper thoracic spine deserves investigation as a potential structural driver contributing to the persistence of symptoms.
When the Elbow Is the Endpoint, Not the Origin
One of the most clinically important patterns in persistent elbow pain is the presence of neck and upper back dysfunction that predates or accompanies the elbow symptoms. Patients often report a history of whiplash, repetitive occupational strain involving the neck and shoulder, or upper limb overuse that follows cervical spine injury. In these cases the elbow pain emerged not from a direct elbow injury but gradually, as motor nerve dysfunction altered the way forearm muscles loaded the tendon over time.
The upper limb functions as a kinetic chain extending from the cervical spine through the shoulder, arm, forearm, and hand. Dysfunction at any point in the chain can concentrate mechanical stress at a more distal location. The elbow is particularly vulnerable as a concentration point because it sits at the junction of the radial nerve distribution from above and the mechanical demands of grip and wrist extension from below. When the cervical nerve supply to the forearm extensors is compromised, the elbow bears the consequence even though the spine is the source.
This pattern also explains why elbow pain in chronic cases frequently travels with neck stiffness, shoulder tension, forearm tightness, and sometimes wrist or hand symptoms. These are not separate complaints. They are different points along the same neuromyofascial chain being affected by the same upstream driver. Mapping that chain from the cervical spine to the lateral epicondyle is what the neuromyofascial investigational process is designed to do.
What We Investigate
→ Cervical spine and cervicothoracic junction dysfunction and which specific segments may be affecting radial nerve motor supply to the forearm extensor muscles.
→ Paraspinal myofibrosis at the cervical and upper thoracic levels as a potential driver of altered motor unit recruitment and persistent forearm extensor dystonia.
→ Radial nerve pathway integrity from the cervical spine through the shoulder and arm to the forearm, and whether tension, sensitization, or compression is present at any point along the chain.
→ Forearm extensor dystonia: whether abnormal sustained hypertonicity in the extensor carpi radialis brevis and related muscles is generating continuous abnormal traction at the lateral epicondyle.
→ Grip strength, forearm coordination, and fine motor control changes suggesting motor neuropathy rather than isolated local tendon inflammation.
→ History of cervical trauma including whiplash, motor vehicle collisions, repetitive occupational neck and shoulder strain, or upper limb overuse following spinal injury that may have initiated the upstream dysfunction.
→ Shoulder girdle involvement including scapular dyskinesis, rotator cuff dysfunction, or thoracic outlet compromise that may be contributing to the kinetic chain dysfunction concentrating load at the elbow.
→ Whether symptoms extend beyond the elbow into the wrist, hand, or fingers, suggesting multi-level upper limb nerve involvement rather than isolated local epicondylalgia.
→ Treatment response history: whether corticosteroid injections, physiotherapy, or surgical release produced only partial or temporary improvement, suggesting the tendon was addressed while the upstream driver remained active.
→ Whether addressing cervical and upper thoracic neuromyofascial dysfunction produces measurable improvement in forearm pain, grip strength, or elbow loading, confirming the spinal contribution to the overall symptom map.
Learn More About Elbow Pain
Below you will find our most comprehensive educational resources on elbow pain and the NMF Science investigational perspective. Explore detailed video explanations, clinical slideshows, and in-depth articles examining the neurogenic contribution to tendinopathy and what neuromyofascial mapping adds to our understanding of chronic lateral epicondylalgia.
Videos
Slideshows