CONDITIONS
Post-Concussion Syndrome (PCS)
Post-concussion syndrome is typically labeled as a brain injury, yet most rehabilitation actually targets the neck, spine, and vestibular system. This paradox reveals something important. Many symptoms called post-concussion may not be purely brain-based. The force of head and neck trauma is often absorbed by the cervical spine, upper back, and connective tissues. Those spinal injuries can generate the exact same symptoms attributed to the brain, including headaches, dizziness, tinnitus, brain fog, and fatigue, while brain imaging remains entirely normal. NMF Science investigates this spinal contribution through a patient-specific neuromyofascial mapping process that standard post-concussion workups are not designed to perform.

Current Medical Understanding
Post-concussion syndrome is described as persistent symptoms following mild traumatic brain injury or concussion. Symptoms typically include headache, dizziness, brain fog, concentration problems, memory difficulty, light and sound sensitivity, tinnitus, fatigue, balance disturbance, and sometimes anxiety or mood changes. Diagnosis relies on symptom history and neurological testing, though brain imaging is frequently normal.
Treatment focuses on brain-centered approaches including cognitive therapy, medications, rest, and symptom management. Many patients improve only partially, or experience worsening symptoms weeks, months, or even years after the original injury. This delayed or progressive pattern is difficult to explain using a simple brain-injury model, and it is one of the central challenges that has led researchers and clinicians to look more carefully at the role of the spine and surrounding soft tissues in driving persistent symptoms.
It is also worth noting a clinical paradox that sits at the center of how PCS is currently managed. Post-concussion syndrome is diagnosed as a brain disorder, yet many of the most effective rehabilitation programs focus heavily on the neck, spine, posture, vestibular function, and musculoskeletal mechanics. The medical system diagnoses the brain. The rehabilitation system often treats the spine. NMF Science proposes that this reflects an underground recognition already present in clinical practice, one that deserves to be made explicit.
NMF Science Perspective
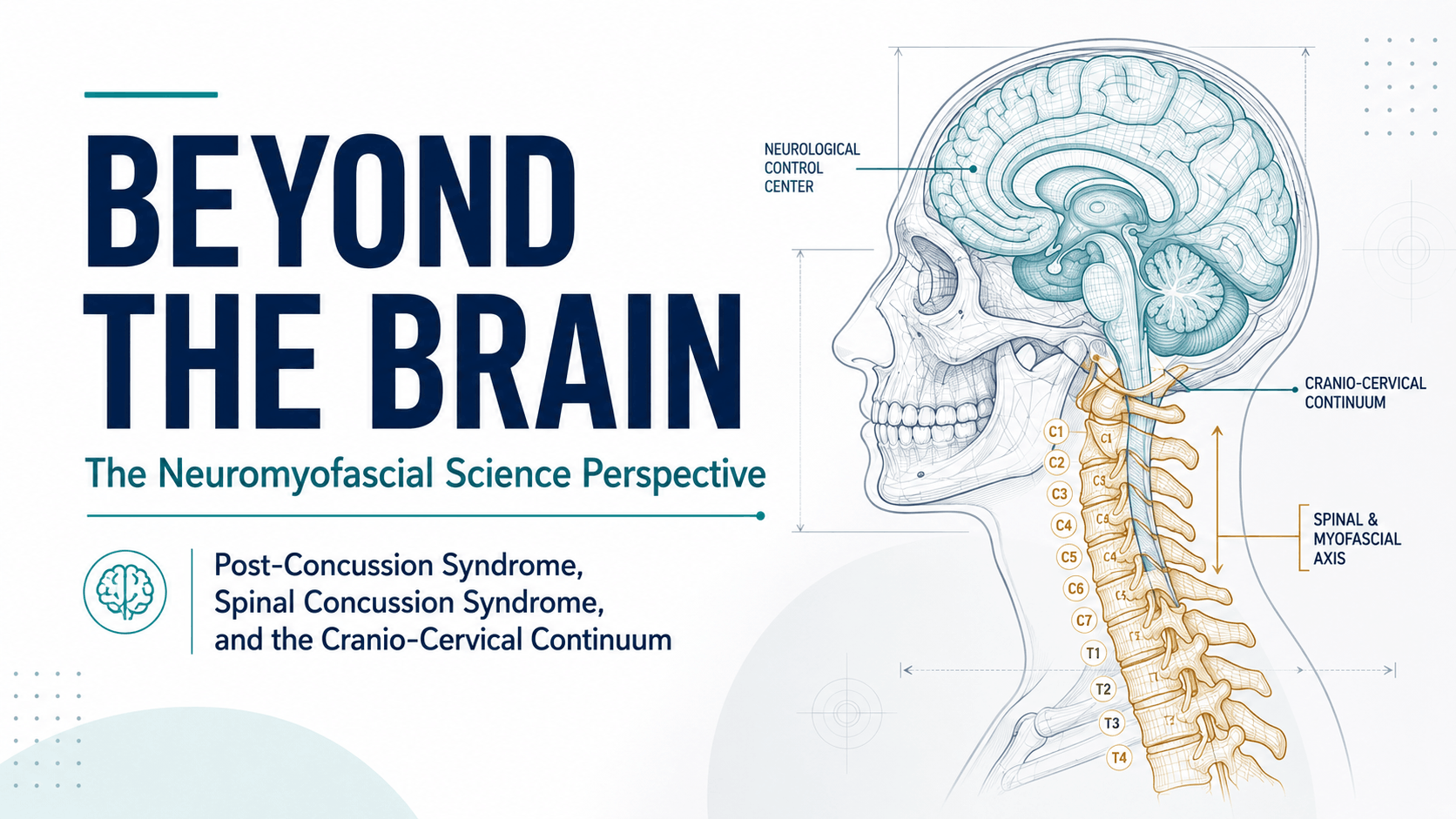
NMF Science proposes that many persistent post-concussion symptoms stem from spinal and neuromyofascial injuries sustained during the original trauma, not from brain injury alone. When the head and neck experience acceleration-deceleration forces, impacts, or rotational trauma, the spine absorbs significant force. The cervical spine and upper thoracic region, particularly the atlas-axis region at C1-C2 at the very top of the neck, are frequent injury sites that standard post-concussion protocols are not designed to fully evaluate.
Dr. G. Blair Lamb introduced the term Spinal Concussion Syndrome, or SCS, to describe this spinal and neuromyofascial contribution to post-concussion symptoms. SCS does not dismiss the possibility of brain injury. A patient may have brain injury, SCS, or both simultaneously. What SCS proposes is that many cases currently labeled as PCS may be better understood as spinal and neuromyofascial disorders generating brain-like symptoms from a physical injury site in the spine rather than from the brain itself.
The mechanism works like this. When the spine experiences trauma, the body responds by forming dense, scar-like neuromyofascial tissue around the injured area to stabilize it. Over time this stabilizing tissue can become pathological, restricting normal spinal movement and creating what is known as spinal cord tethering. When the spinal cord cannot glide freely during movement, it creates physical tension that radiates upward toward the brainstem, cranial nerves, optic nerve, and brain.
This tethering mechanism explains how a spinal injury produces symptoms that look identical to brain injury: headaches concentrated at specific locations, vestibular disruption including dizziness and vertigo, visual disturbance and light sensitivity, tinnitus and auditory symptoms, brain fog and concentration difficulty, fatigue, mood changes, and autonomic symptoms. The wide variability in symptoms between patients reflects where each person's spine absorbed the injury force. Symptoms are not random. In the NMF Science framework they are specific clues pointing to localized injured regions along the spinal column.
The C1-C2 atlas-axis region is particularly important. This upper cervical junction governs head position and balance mechanics, making it a primary generator of craniofacial pain, severe headache, and vestibular disruption when injured. Standard MRI is not designed to visualize the microscopic neuromyofascial scarring that occurs here, and hypermobile patients present a particular diagnostic challenge because their natural joint flexibility can easily mask the loss of motion occurring deeper in the tissue.
Delayed or progressive symptoms, where patients worsen weeks or years after the original injury, fit the SCS model better than the brain-injury model. As scar tissue progressively tightens, it further restricts spinal cord mobility and increases neural tension. What begins as a localized cervical injury can expand into a whole-injury pattern affecting the brainstem, cranial nerves, optic nerve, and autonomic nervous system over time.
When Symptoms Are Misread as Psychiatric
One of the most consequential patterns in post-concussion care is the misattribution of neurological symptoms to psychiatric causes. Brain fog, crushing fatigue, anxiety, depression, and PTSD-like features are frequently treated with psychiatric medication in patients whose underlying driver is physical traction deep within the spinal canal.
In the NMF Science framework, mood and cognitive symptoms in PCS patients are often neurological side effects of sustained spinal cord tension rather than primary psychiatric conditions. When that spinal tension is identified and addressed through precise neuromyofascial mapping, some patients report improvement in mood, cognitive clarity, and fatigue alongside their physical symptoms. This does not mean psychiatric care is never appropriate. It means the spinal contribution to these symptoms deserves investigation before assuming the problem is entirely psychological.
Treatment response is itself a mapping tool. If releasing a specific restriction in the cervical spine immediately reduces a patient's vertigo or clears their headache, the clinician has successfully mapped that symptom back to its anatomical driver. Recovery in the SCS model happens systematically, by identifying and addressing each layer of the injury pattern rather than managing symptoms at the surface level.
What We Investigate
→ The mechanism of injury including whiplash, acceleration-deceleration forces, direct impact, sports trauma, and repeated impacts, and where in the spine that force was most likely absorbed.
→ Atlas-axis region integrity at C1-C2 and upper cervical spine involvement as a primary driver of headache, craniofacial pain, and vestibular symptoms.
→ Spinal cord tethering: whether dense neuromyofascial scarring is restricting normal cord glide and generating upward neural tension toward the brainstem and optic nerve.
→ Timing and progression of symptoms: whether immediate, delayed, or progressive onset patterns suggest spinal rather than purely brain-based pathology.
→ Specific symptom patterns including headache location, one-sided versus bilateral tinnitus, positional dizziness, and visual disturbance, as anatomical clues pointing to localized spinal injury sites.
→ Cervical and upper thoracic range of motion, segmental restriction, vertebral alignment, and signs of fibrosis or scar tissue formation at key injury sites.
→ Hypermobility as a diagnostic blind spot: whether normal or excessive range of motion is masking serious spinal malalignment or deeper tissue injury.
→ Whether mood, cognitive, and fatigue symptoms may represent neurological effects of spinal cord tension rather than primary psychiatric conditions.
→ History of prior injuries, repeated trauma, sports impacts, or accident patterns that may have compounded spinal damage over time before the most recent concussive event.
→ Whether standard imaging fully explains the symptom pattern, or whether the patient's neuromyofascial map points to injury that current MRI protocols are not designed to capture.
Learn More About Post-Concussion Syndrome
Below you will find our most comprehensive educational resources on Post-Concussion Syndrome and Spinal Concussion Syndrome from the NMF Science perspective. Explore detailed video explanations, clinical slideshows, podcasts, and in-depth articles examining the spinal and neuromyofascial contribution to persistent post-concussion symptoms.
Videos
Slideshows