Post-concussion syndrome is one of the more poorly understood conditions in medicine. Patients present with headaches, dizziness, tinnitus, brain fog, light sensitivity, and fatigue. Imaging comes back normal. The diagnosis is brain-centered, yet many of the rehabilitation approaches that actually help these patients are focused on the neck, spine, and vestibular system.
This paradox is not a coincidence. It reflects something that has been sitting in clinical practice for years without being made fully explicit: in many cases, what is labeled as post-concussion syndrome is better understood as a spinal and neuromyofascial disorder.
I introduced the term Spinal Concussion Syndrome, or SCS, to name and describe this spinal contribution to post-concussion symptoms. This article explains what SCS is, why it is clinically distinct from brain-based PCS, and why the difference matters for recovery.
What Post-Concussion Syndrome Gets Wrong
The standard model of post-concussion syndrome treats the brain as the primary injury site. A concussive event occurs, the brain is assumed to be the damaged tissue, and treatment is directed accordingly: cognitive therapy, rest, medications, and symptom management.
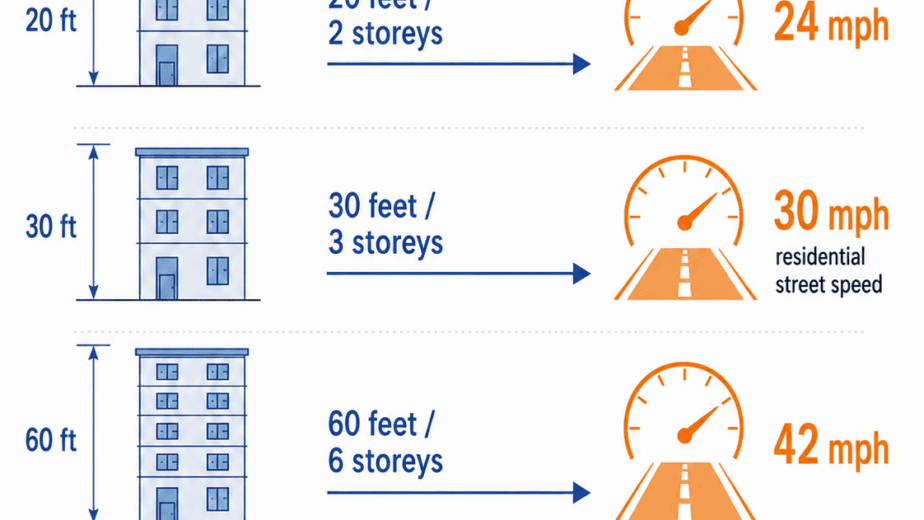
This model works reasonably well for some patients. For many others it does not, and the reason is straightforward. A concussive event is rarely a brain-only event. When the head undergoes acceleration-deceleration forces, whether from a motor vehicle accident, a contact sport impact, a fall, or a direct blow, the cervical spine absorbs a significant portion of that force. The neck and the head move together. The brain and the spine are injured together.
When the cervical spine is not investigated as part of the post-concussion workup, a major injury site is being left out of the picture. The symptoms that follow may then be attributed entirely to the brain when their actual driver is the spine.
Three clinical patterns make this clearer. First, symptom severity frequently does not match the force of the original impact. Minor impacts sometimes produce severe, persistent symptoms while more dramatic traumas produce less. If symptoms were purely the result of brain tissue damage, you would expect a more consistent relationship between impact force and symptom severity. Second, some patients develop post-concussion symptoms after acceleration-deceleration injuries with no direct head strike at all. This is very difficult to explain as a brain injury. Third, symptoms frequently worsen or emerge weeks or months after the original event. Classic brain injury typically peaks at day one and then gradually improves. Delayed escalation suggests a different physiological process.
All three patterns fit more naturally with a spinal injury model than with a brain injury model.
The Mechanism: Spinal Cord Tethering
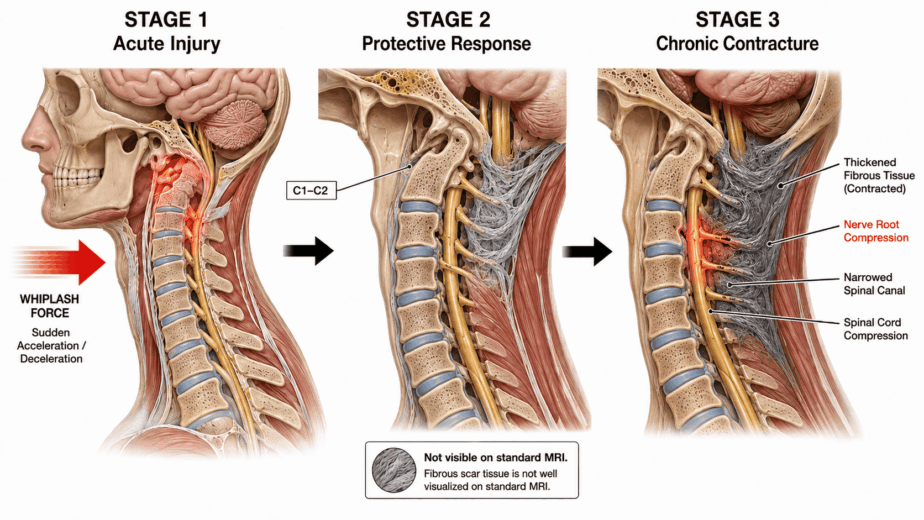
When the spine experiences trauma, the body responds by forming dense scar-like neuromyofascial tissue around the injured area. In the short term, this is a protective mechanism. The tissue stabilizes the injured region, functioning as a kind of internal brace.
Over time, however, this stabilizing tissue can become pathological. As it accumulates and matures, it restricts normal spinal movement and, critically, it can begin to tether the spinal cord. The spinal cord is designed to glide freely within the spinal canal during movement. When surrounding scar tissue anchors it in place, normal movement creates tension along the cord itself.
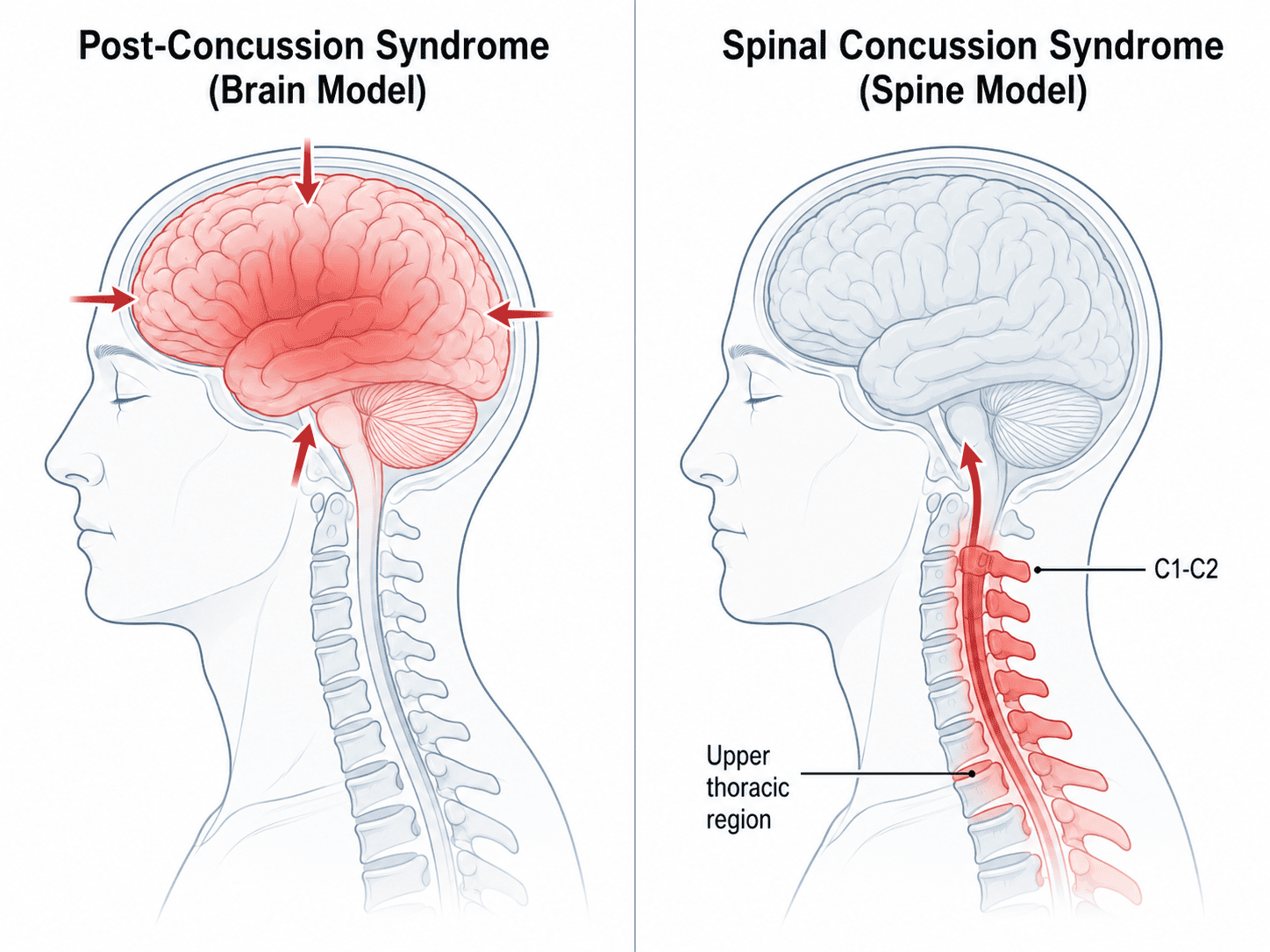
That tension does not stay localized. It transmits upward through the cord toward the brainstem, cranial nerves, optic nerve, and into the skull. This is the mechanism by which a spinal injury generates what looks exactly like a brain injury: headaches concentrated at specific locations, vestibular disruption including dizziness and vertigo, visual disturbance and light sensitivity, tinnitus, cognitive changes including brain fog and difficulty concentrating, fatigue, mood changes, and autonomic symptoms.
The upper cervical region, specifically the atlas-axis junction at C1-C2, is particularly important in this process. This region governs head position, balance mechanics, and the transition point between the spinal cord and the brainstem. Injury here can generate severe craniofacial pain, intractable headache, and significant vestibular disturbance. It is also a region that standard post-concussion protocols are not designed to evaluate in detail.
SCS Does Not Replace PCS
Spinal Concussion Syndrome is not an argument that brain injury never occurs. A patient can have brain injury without SCS, SCS without direct brain injury, or both simultaneously. The clinical picture is not always one or the other.
What SCS proposes is that many cases currently labeled as post-concussion syndrome are driven substantially or entirely by spinal and neuromyofascial injury rather than by the brain. In those cases, brain-centered treatment will produce incomplete results because the actual injury site is not being addressed.
The practical implication is that the spinal contribution should be investigated and mapped as part of any thorough post-concussion workup, not left as an afterthought or assumed to be normal because standard imaging does not show it.
Spinal cord tethering, craniocervical fibrosis, and deep cervical muscle injury at the levels described above are not reliably visible on standard MRI protocols. They require a more detailed investigational approach: one that maps the mechanism of injury, traces symptoms back to likely spinal origins, and treats what is found rather than managing symptoms at the surface.
Why Recovery Stalls
The patients who do not recover with standard post-concussion rehabilitation have often been told there is nothing more to offer, that their symptoms are driven by anxiety, central sensitization, or lingering neurological effects of the brain injury itself.
In many of these cases, the missing piece is the spinal injury. The cord tethering, the craniocervical fibrosis, the upper cervical compression: these are not being identified or treated. Rehabilitation that targets brain function cannot resolve them because they are structural tissue problems, not functional brain problems.
Recovery in the SCS model happens by identifying and addressing each layer of the spinal and neuromyofascial injury pattern systematically. The treatment approach through TNPC targets the fibrotic tissue, releases cord tethering, and decompresses the affected spinal segments. In patients whose symptoms have been labeled as permanent post-concussion syndrome, this approach has produced meaningful and in some cases complete recovery.
The brain is not always the primary problem. In many post-concussion patients, it is the spine.
The information in this article is educational and informational in nature. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. If you are experiencing post-concussion symptoms or chronic head and neck pain following an injury, consult with a qualified healthcare provider to discuss the options appropriate for your situation.