When a spinal injury heals, most people assume the tissue returns to something close to its original state. Scar forms, the acute phase resolves, and the body moves on. For a significant number of whiplash patients, that is not what happens. The body’s repair response produces something structurally different from the tissue it replaced, and in some cases, that new tissue creates more problems than the original injury.
Dr. G. Blair Lamb describes this process through the concept of super contractures: dense, organized bands of neuromyofascial scar tissue that form around injured spinal segments in the weeks and months following trauma. Understanding what these are, how they form, and why standard imaging cannot see them is essential to understanding why so many whiplash patients do not recover.
The Evolutionary Injury Response
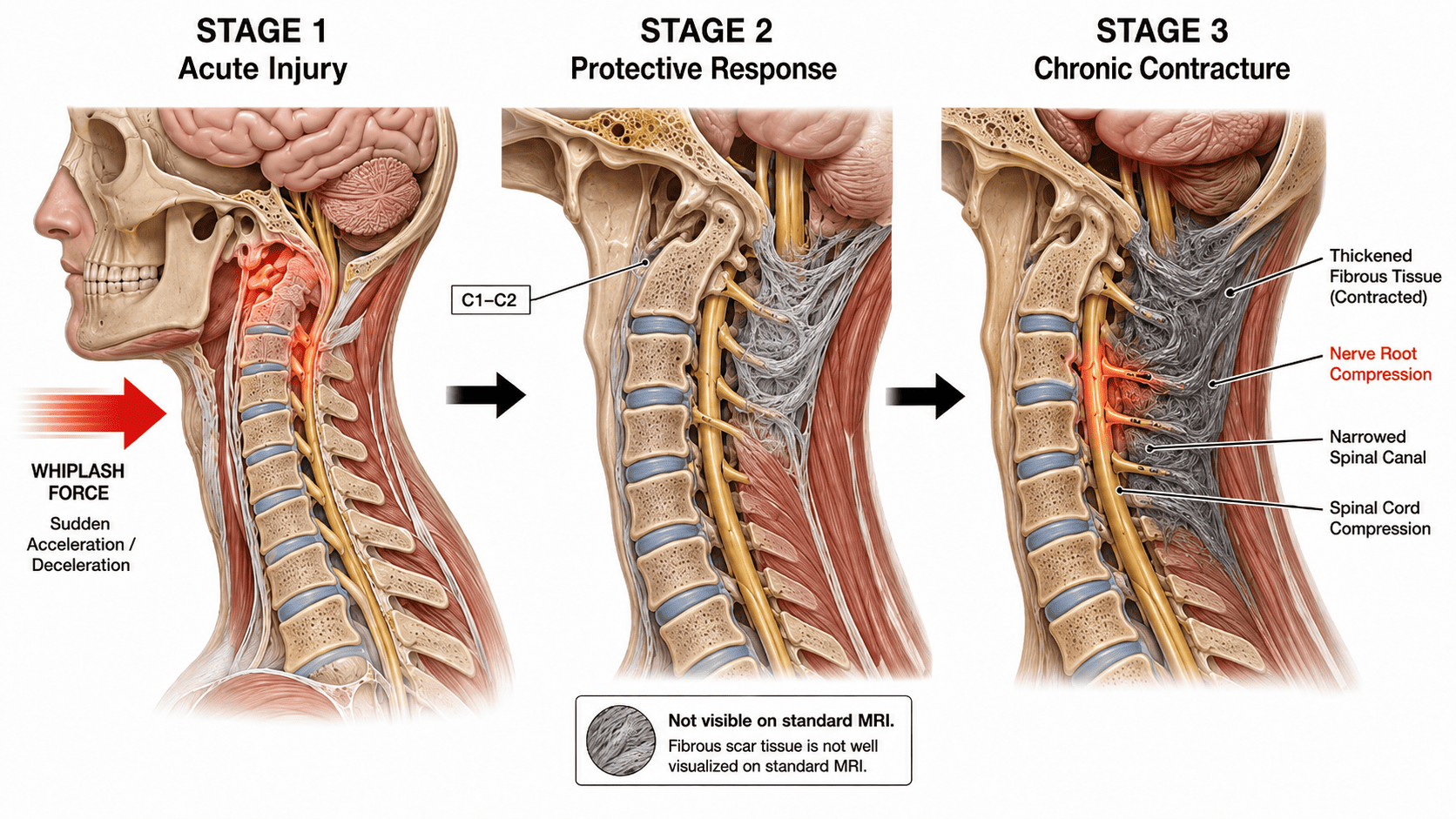
When the spine sustains significant trauma, the body initiates what Dr. Lamb describes as the evolutionary injury response. It is a survival mechanism. The body detects structural instability in the injured region and responds by rapidly forming dense, fibrous stabilizing tissue around the damaged vertebrae and soft tissue. The goal is to create an internal cast, to immobilize the injured segment and prevent further damage.
In an acute setting, this response is protective and appropriate. In the short term, stabilizing a damaged spinal segment through fibrous tissue formation helps prevent the kind of secondary cord injury that movement through an unstable region could cause.
The problem emerges over time. As the stabilizing tissue matures, it can become progressively denser, more disorganized, and more contractile. What began as a protective internal cast transitions into a pathological structure. The tissue shrinks and tightens. It locks spinal vertebrae out of their natural alignment. It compresses the surrounding nerve roots. And in its most advanced form, it wraps around the spinal cord itself, restricting the normal gliding motion the cord depends on during movement.
This is the super contracture. Tissue that was formed to protect the spine has become the mechanism of chronic injury.
Why Standard Imaging Cannot See It
Standard MRI, X-ray, and CT scanning are designed to detect structural abnormalities: fractures, disc herniations, obvious soft tissue masses, gross alignment changes. They are not designed to detect the subtle density changes, fascial contractures, and dynamic restriction patterns that characterize neuromyofascial super contractures.
The result is a diagnostic blind spot that affects millions of patients. A whiplash patient with significant spinal neuromyofascial scarring undergoes standard imaging, receives a report showing no significant abnormality, and is told their spine is essentially normal. The super contractures generating their pain and neurological symptoms are present but invisible to the tools being used to look for them.
Curatolo and colleagues (2011) addressed this directly in a review of tissue damage in whiplash-associated disorders, concluding that “lack of macroscopically identifiable tissue damage does not rule out the presence of painful lesions.” They argued that pain-generating lesions may be microscopic, may exist below imaging resolution, and that the absence of visible pathology on standard imaging does not exclude clinically significant structural injury.
This is not a failure of imaging technology for the purposes it was designed for. It is a mismatch between what the technology can detect and what is actually driving the patient’s symptoms.
Spinal Cord Tethering: When the Cast Becomes a Cage
Normally, the spinal cord glides freely within the spinal canal as the body moves. This gliding motion is essential for normal neurological function. When dense neuromyofascial scarring accumulates around the cord, it restricts that glide. The cord becomes tethered.
A tethered spinal cord does not simply stay still. It transmits tension. Every movement that would normally allow the cord to glide instead generates mechanical tension along its length. That tension does not stay localized. A tethering point at the upper cervical spine can transmit upward tension into the brainstem and cranial nerves. It can pull downward, generating unexplained weakness or heaviness in the legs. It can create the persistent headaches, vestibular disruption, visual changes, fatigue, brain fog, and sensory disturbances that whiplash patients describe and that brain-centered assessment cannot explain.
Research in analogous conditions including adhesive arachnoiditis, tethered cord syndromes, and post-surgical spinal adhesions has documented neurological symptoms including pain, sensory disturbances, weakness, balance dysfunction, and fatigue arising from restricted neural mobility rather than gross compression. The specific mechanism of post-whiplash fibrosis producing spinal cord tethering as described by Dr. Lamb is a clinical hypothesis that warrants dedicated investigation. The biological plausibility of neural tissue becoming mechanically sensitized by adhesions and altered mobility is well established in this broader literature.
This mechanism helps explain why whiplash symptoms often worsen over time rather than improving. The acute injury event initiates the evolutionary injury response. The repair tissue forms and matures over the following weeks, months, and years. As it tightens and contracts, the cord tethering increases and the symptom picture worsens. The patient deteriorates after an injury event that occurred years earlier, and the connection between the two is missed because no one is looking at what the repair process left behind.
Elliott and colleagues demonstrated in serial MRI investigations that patients with persistent whiplash symptoms showed significantly greater deep cervical muscle degeneration, fatty infiltration, and structural tissue remodeling than patients who recovered. The degree of chronic tissue change tracked with symptom persistence rather than resolving with time, supporting the concept that a pathological remodeling process continues in patients who do not recover.
The Kinetic Energy Factor
Dr. Lamb has noted, as discussed in the physics of whiplash, that the forces involved in motor vehicle accidents are routinely underestimated by patients, clinicians, and insurers alike. Highway speed collisions generate deceleration forces equivalent to falling from a twelve-storey building. Even residential speed impacts involve forces the human body was not designed to absorb without tissue injury.
Siegmund and colleagues (2001) demonstrated that cervical facet capsular ligaments can sustain injury under whiplash loading conditions through combined compression, shear, and extension forces, and that this injury can occur without fractures or major MRI findings. This is a biomechanical parallel to the broader neuromyofascial argument: significant tissue injury occurs at force levels that leave no obvious trace on standard imaging.
The severity of the super contracture response relates directly to the force absorbed by the spine. Higher-force injuries produce more extensive neuromyofascial scarring, greater contracture density, and more significant cord tethering. This is why some patients involved in apparently minor accidents develop severe, progressive chronic pain syndromes while others recover. The tissue response depends on the force absorbed, the pre-existing condition of the spinal tissues, and individual biological variation in how the repair process organizes.
The Opioid Connection
The relationship between undiagnosed and untreated spinal neuromyofascial injury and the opioid crisis is not a peripheral concern. It is a direct consequence of a diagnostic gap.
When a patient with significant spinal super contractures and cord tethering receives a normal MRI result, the clinical pathway typically moves toward pain management rather than structural investigation. Medications are prescribed. In severe cases, opioid therapy is initiated. The underlying structural problem driving the pain remains unidentified and unaddressed.
The scale of this problem is substantial. A Mayo Clinic review of whiplash-associated disorders found that up to 50 percent of patients report persistent symptoms months to years after the initial injury, with up to 30 percent experiencing moderate-to-severe chronic pain and disability. When that proportion of patients is offered only symptom management because structural investigation has been closed by a normal MRI result, the conditions for long-term dependency are created by the diagnostic gap rather than by patient behavior.
Long-term pain management without resolution of the structural driver is a reliable pathway toward dependency. A patient in persistent severe pain has a legitimate medical reason to seek relief. When the only tools offered are pharmacological, and when those pharmacological tools manage symptoms without addressing their source, the opioid pathway opens not through failure of will but through failure of investigation.
The clinical argument for better identification and treatment of spinal neuromyofascial pathology after whiplash is not only about individual patient outcomes. It is about addressing a systemic failure in how these injuries are assessed and managed at the population level.
What This Means for Patients
Patients who have been told their imaging is normal following a whiplash injury, who continue to experience pain and neurological symptoms that do not respond to standard rehabilitation, and who have been offered only symptom management deserve a different question: what did the injury leave behind that standard imaging cannot see?
The super contracture model provides a mechanistically coherent answer. The evolutionary injury response formed protective tissue. That tissue matured into a pathological structure. The structure is generating the symptoms. Identifying it, mapping it accurately, and addressing it through precisely targeted intervention is how the clinical ceiling that symptom management cannot break through gets lifted.
The biological concepts underlying this model are supported by a growing body of peer-reviewed evidence. The specific terminology and the full causal chain as Dr. Lamb describes it remain investigational. That is not a reason to dismiss the framework. It is a reason to investigate it.
This article draws on the clinical framework of Dr. G. Blair Lamb and is intended for educational purposes. It is not a substitute for professional medical advice, diagnosis, or treatment. If you are experiencing chronic symptoms following a whiplash injury that have not responded to standard care, consult with a qualified healthcare provider.
This topic is explored in depth in Episode 003 of the Neuromyofascial Science Today podcast. Listen on Spotify.