Carpal tunnel syndrome is one of the most commonly diagnosed and surgically treated conditions in upper limb medicine. The standard model is straightforward: the median nerve is compressed within the carpal tunnel at the wrist, producing numbness, tingling, and weakness in the thumb, index, middle, and part of the ring finger. Decompress the tunnel and the symptoms resolve.
For many patients, that model is incomplete. A significant proportion of people who undergo carpal tunnel release either do not fully recover or eventually relapse. In many of those cases, the reason is that the wrist was not where the problem originated.
The Nerve Runs from the Neck to the Hand
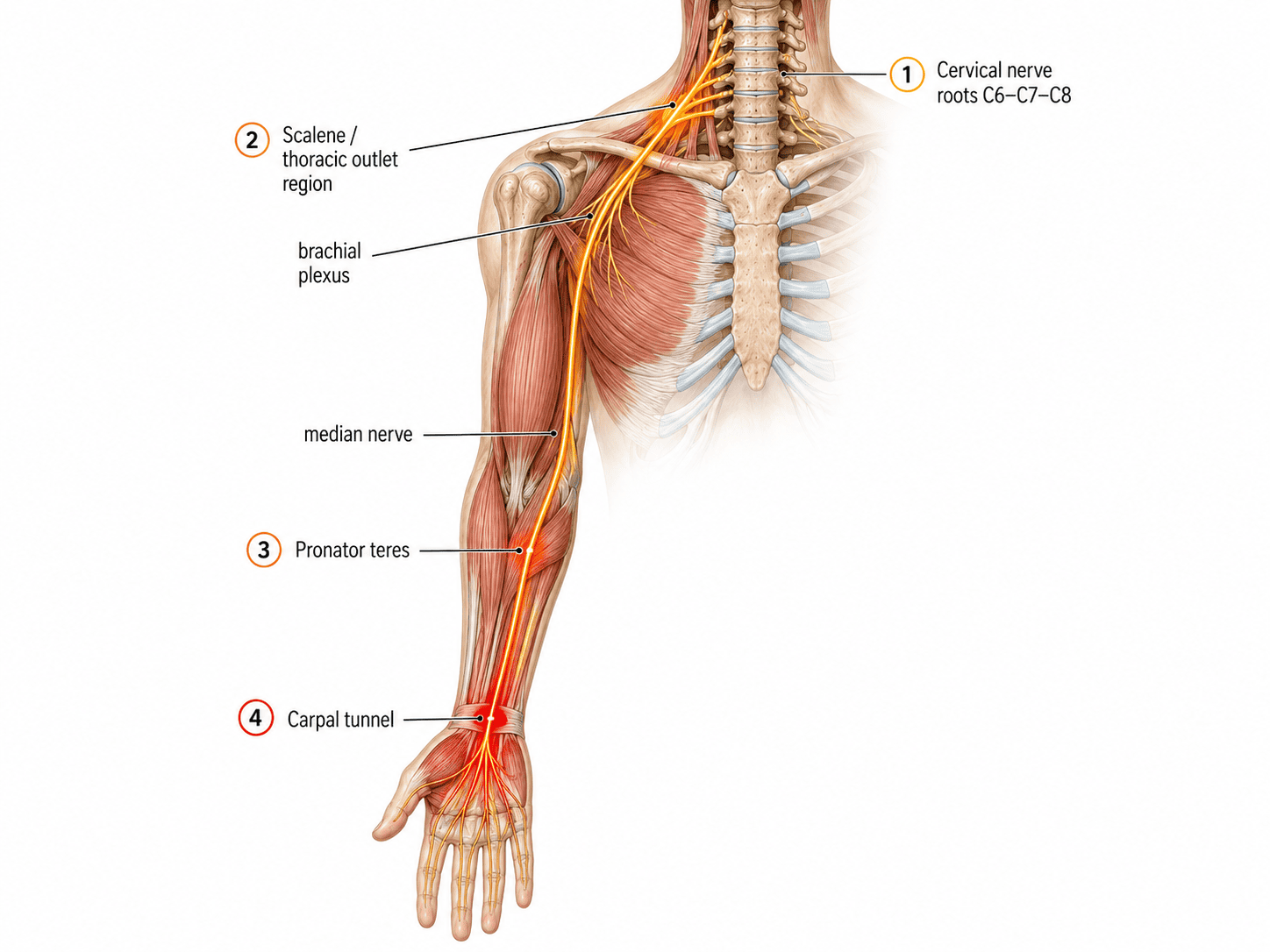
The median nerve does not begin at the wrist. It originates from nerve roots in the lower cervical spine, primarily C6, C7, and C8, and travels through the brachial plexus, across the shoulder, down through the forearm, and into the hand. Any point along that pathway where the nerve is compressed, tethered, or subjected to chronic traction becomes a potential contributor to median nerve symptoms in the hand.
This is the core concept behind what the research literature describes as double crush syndrome: the idea that a nerve under proximal compression becomes more vulnerable to symptomatic injury at a distal site. First described by Upton and McComas in The Lancet in 1973, their study of 115 patients with carpal tunnel syndrome or ulnar nerve lesions found that 81 had electrophysiologic evidence of associated neural lesions in the neck. The association, they concluded, was not coincidental.
More recent epidemiological support comes from a 2024 retrospective cohort study published in Global Spine Journal by Mills and colleagues, which analyzed surgically treated patients across a large database. Among patients with cervical radiculopathy, approximately 10 percent had concurrent CTS and 3 percent had concurrent peripheral ulnar nerve compression. The association was bidirectional: patients with CTS were also significantly more likely to have cervical radiculopathy than matched controls. This bidirectional pattern is consistent with the neuromyofascial model of multi-level nerve involvement rather than isolated distal entrapment.
How the Cervical Spine Creates a Wrist Problem
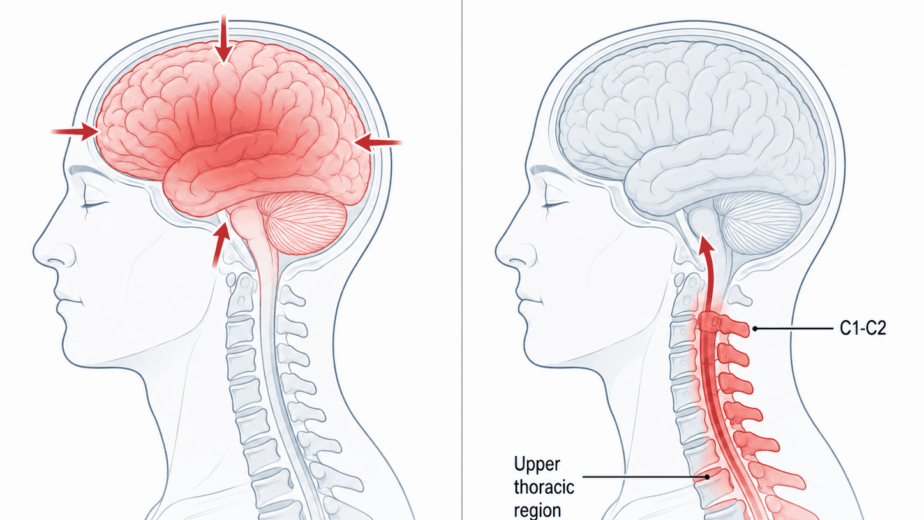
The injury sequence typically begins in the cervical spine, often from a whiplash event, repeated neck strain from prolonged desk work, or cumulative upper back injury. High-density neuromyofascial scar tissue accumulates in the lower cervical region, often not visible on standard MRI, and begins to compress or irritate the nerve roots supplying the arm.
That nerve root compression creates a motor neuropathy: partial impairment of the motor nerve signal traveling down the arm. The muscles supplied by those nerve roots, including certain neck muscles, shoulder girdle muscles, scalene muscles, and eventually the forearm muscles, begin to lose normal tone regulation. They progressively shorten and develop dystonia.
The scalene muscles in the neck and the pectoralis minor in the chest wall are of particular clinical relevance here. As these muscles develop chronic tightness and shortening, they create compression and tethering of the brachial plexus as it passes through the neck and shoulder region. This is the thoracic outlet component, supported in the literature by Sanders and Annest, whose clinical review established that proximal soft tissue compression at the scalene and pectoralis minor regions can generate upper limb pain, numbness, tingling, and weakness that may be misidentified as isolated distal entrapment.
Further down the arm, the pronator teres and pronator quadratus muscles in the forearm, also under the influence of compromised cervical nerve supply, develop tightness that creates additional compression points along the median nerve’s course before it even reaches the wrist. A 2022 review in the Journal of Clinical Medicine by Löppönen and colleagues confirmed that proximal median nerve compression can fully mimic carpal tunnel syndrome symptomatically and may contribute to persistent symptoms after wrist decompression in patients where the proximal component was not identified.
By the time the median nerve reaches the carpal tunnel, it is arriving under chronic traction from multiple proximal tethering sites. The nerve is less mobile than it should be. Research using dynamic ultrasound, reviewed systematically by Huang and colleagues in 2022, has demonstrated measurably reduced median nerve mobility in CTS patients, supporting the concept that impaired nerve gliding and tissue tethering contribute meaningfully to symptoms alongside static wrist compression.
The carpal tunnel, in this sequence, is the last pinch point on an already compromised nerve. Releasing that pinch without addressing what has been loading the nerve from above may produce temporary relief, but the underlying traction mechanism remains active.
Ulnar Neuritis Follows the Same Logic
The ulnar nerve, which supplies the little finger and ring finger and originates from C7 through T1, follows a parallel course through the same cervical and thoracic outlet territory. Ulnar neuritis, in which the nerve is entrapped at the elbow, shows the same pattern of proximal contribution seen in CTS.
A case-control study by Smith and colleagues published in the Clinical Journal of Sport Medicine found that cyclists with clinical ulnar nerve neuropathy had significantly more proximal dysfunction findings: neck pain was approximately three times more common, shoulder pain five times more common, and elevated first rib findings twelve times more common compared to controls without ulnar symptoms. The proximal pattern was consistent and significant.
In the neuromyofascial model, ulnar neuritis frequently involves contractures and trigger points in the latissimus dorsi and triceps muscles that create traction on the ulnar nerve as it transitions toward the elbow. Addressing these upstream contributors alongside the local elbow entrapment is what determines whether recovery is complete or partial.
When Surgery Is and Is Not Sufficient
Surgical carpal tunnel release remains appropriate and necessary in cases where the nerve compression at the wrist is severe, where there is significant motor loss or muscle wasting, or where the condition is acute and progressive. The clinical literature does not support delaying surgery in urgent presentations.
What the literature does support, and what clinical observation at the NMF Science clinic has consistently demonstrated, is that many less severe or recurrent CTS presentations have a significant proximal component that surgery at the wrist alone will not resolve. In those cases, targeted neuromyofascial investigation of the cervical spine, thoracic outlet, shoulder girdle, and forearm identifies the tethering sites loading the median nerve from above. Through TNPC, addressing those sites reduces the chronic traction on the nerve, allowing the carpal tunnel itself to decompress without the sustained abnormal tension that produced the original entrapment.
The wrist is where the symptoms are. The neck, in many cases, is where the problem began.
The information in this article is educational and informational in nature. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. If you are experiencing symptoms of carpal tunnel syndrome or upper limb nerve pain, consult with a qualified healthcare provider to discuss the diagnostic and treatment options appropriate for your situation.