Plantar fasciitis is one of the most commonly treated foot conditions and one of the most commonly undertreated. Stretching, orthotics, corticosteroid injections, and rest produce temporary relief for many patients but do not produce lasting recovery. The reason, in most chronic cases, is straightforward: the treatment is being directed at the endpoint of the problem, not the source.
Nearly three decades of clinical research and patient care have consistently shown that plantar fasciitis is driven, in whole or in part, by injury patterns in the lumbar spine, sacrum, pelvis, hip, and calf. When those upstream sites are not identified and addressed, local treatment will manage symptoms for a period and then the pain returns. The foot is the alarm. The spine and lower limb chain are where the problem originates.
The Kinetic Chain from Spine to Sole
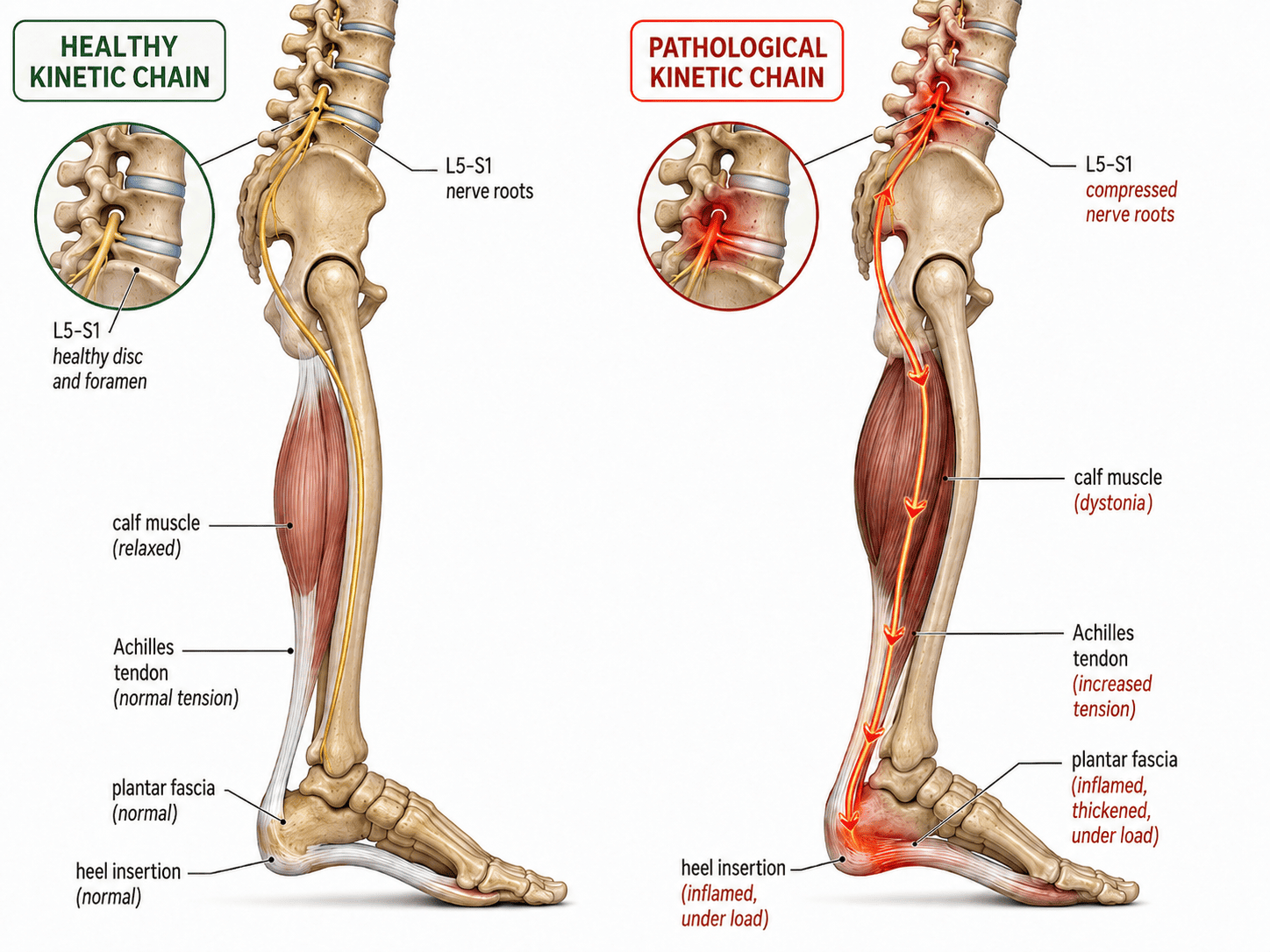
The lower limb functions as a continuous mechanical chain. Nerve roots exiting the lumbar and sacral spine travel down through the hip, thigh, calf, and into the foot. When those nerve roots are compressed or irritated, whether from disc pathology, fibrosis, or neuromyofascial scarring at the lumbar or sacral levels, the effects travel the full length of the chain.
The most common mechanism works like this. Nerve root compression at L5 or S1 creates motor neuropathy in the muscles it supplies, particularly the calf. The gastrocnemius and soleus respond with dystonia, a state of chronic involuntary tension in the muscle. A dystonic calf does not simply feel tight. It is mechanically shortened, functioning like a pulley under constant load. That constant load transmits upward tension through the Achilles tendon and downward tension into the plantar fascia at the heel and arch.
The plantar fascia, caught at the end of this tensioned chain, develops inflammation and microtearing at its attachment point on the calcaneus. That is what produces the characteristic heel pain on first steps out of bed in the morning. But the fascia is not the generator. It is absorbing force that has been building from L5 and S1 downward through a progressively tightened kinetic chain.
Treating the plantar fascia without addressing the calf dystonia and its lumbar or sacral source leaves the mechanical force generator fully active. The fascia may settle temporarily with rest and local treatment. The moment normal loading resumes, the same abnormal tension pattern recreates the same injury.
The Layers of the Problem
Simple presentations of plantar fasciitis may involve only the lumbar or sacral spine and the bottom of the foot. These cases often respond well to targeted spinal care combined with local foot and calf rehabilitation.
Chronic and more complex presentations tend to involve multiple regions simultaneously. In these cases the injury map typically spans the lower lumbar spine or sacrum, the pelvic and hip musculature, the hamstrings, the calf, and the foot itself. Each region contains sites of dystonia or fibrosis that are contributing to the abnormal tension being loaded onto the plantar fascia. For full recovery, all of those contributing sites need to be identified and addressed, not just the most symptomatic one.
Hip musculature is a frequently overlooked driver. The piriformis, gluteus medius, and related pelvic muscles, when in a state of chronic spasm or scarring, alter lower limb alignment and loading mechanics through the entire leg. This altered mechanics compounds the lumbar nerve root contribution to calf tightening and plantar fascia strain.
Achilles tendinitis and plantar fasciitis frequently occur together because they share these upstream drivers. The same dystonic calf that loads the plantar fascia also tethers the Achilles tendon. Finding one should prompt investigation of the other and, more importantly, investigation of what is generating the calf dysfunction in the first place.
When the Foot Is Not Even the Right Place to Look
In a smaller but clinically significant subset of cases, plantar fasciitis has persisted despite exhaustive local treatment, thorough lumbar and sacral workup, and hip rehabilitation. In these cases, neuromyofascial investigation has identified contributing pathology in the upper thoracic or cervical spine.
This may seem counterintuitive. The cervical spine and the plantar fascia are anatomically distant. The connection becomes more logical when you understand that the spinal cord runs continuously from the brainstem to the lumbar spine, and that myelopathic changes, meaning irritation or dysfunction at the level of the spinal cord itself, can generate motor abnormalities in the limbs that are far removed from the site of the cord involvement.
In documented cases at the clinic, cervical and upper thoracic myelopathic contributions to plantar fasciitis have been identified. When those regions were treated and the myelopathic contribution resolved, the chronic plantar fasciitis resolved as well, without any direct intervention to the foot.
These are not typical presentations. Most plantar fasciitis does not require cervical spine investigation. But in the genuinely treatment-resistant patient who has tried every local approach without result, the full spinal picture deserves investigation.
What Investigation and Treatment Address
A thorough neuromyofascial investigation of chronic plantar fasciitis maps each potential contributing site from the lumbar and sacral spine downward through the hip, pelvis, hamstring, calf, and foot. The goal is to identify which sites are active contributors and in what sequence they are loading the plantar fascia.
Through TNPC, targeted interventions address the neuromyofascial pathology at each identified site rather than managing the foot symptoms in isolation. Spinal nerve root decompression, calf and hip dystonia treatment, and local plantar fascia work are sequenced according to the injury map rather than applied by a generic protocol.
In straightforward cases, targeted spinal and lower limb care produces complete resolution. In more complex multi-region presentations, recovery takes longer and requires working through the full injury chain systematically. In both cases, the outcome depends on correctly identifying where the force driving the plantar fascia is actually coming from.
Plantar fasciitis that keeps coming back is not a stubborn foot problem. It is an investigation problem.
The information in this article is educational and informational in nature. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. If you are experiencing chronic foot pain or plantar fasciitis that has not responded to standard treatment, consult with a qualified healthcare provider to discuss the options appropriate for your situation.