When a patient describes waking up with a stiff neck, a migraine by noon, a numb hand by evening, and a familiar ache down the leg, the standard medical response routes each symptom through a different door. A neurologist for the head. An orthopedist for the hand. A pain specialist for the back. Each clinician assigns a label. Each label generates a treatment. And the patient returns home carrying five separate diagnoses, five separate explanations, and often, very little resolution.
I have spent more than thirty years examining that pattern, and I no longer believe those five symptoms are separate problems.
The neuromyofascial science framework I developed is built around a different premise: that many of the most common and persistent pain presentations are connected expressions of one underlying physical process. The symptoms look different because they surface in different parts of the body. But the architecture producing them is often unified.
Understanding that architecture changes what you look for, and where.
What Is Acquired Neuromyofascial Pathology?
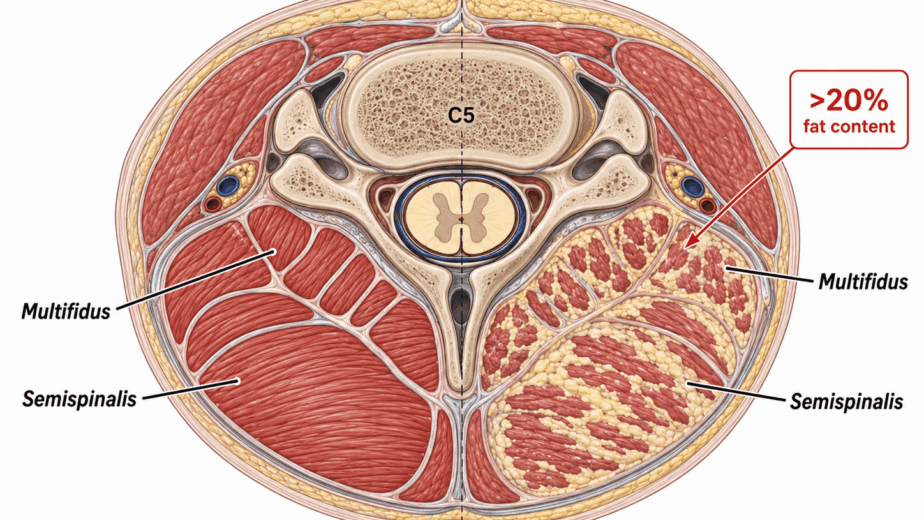
The central concept in this framework is what I refer to as acquired neuromyofascial pathology. This is not a single injury event. It is a cumulative process. Over years and decades, invisible microinjuries accumulate in predictable regions of the spine and limbs. Scar tissue forms. The density of the affected connective tissue increases. And that increased density begins to have mechanical consequences: altered spinal positions, compressed joints, and irritation of the delicate nerve roots passing through the region.
The process is slow, quiet, and almost entirely invisible on standard imaging. Because the damage lives in soft tissue density rather than in bone or disc, routine MRI and X-ray are poorly suited to detect it. Patients come in with real, measurable physical pathology that does not show up on the scans used to look for it. The scan comes back clean, and the clinical response is often some variation of: this is just a normal part of getting older.
Fifty is still fifty. Sixty is still sixty. But the pain you are feeling is not always explained by age alone. In a meaningful proportion of cases, that pain is the result of mechanical, structural burden that has been silently compounding for years.
Fascia Is Not Passive Wrapping
For a long time, the connective tissue scaffolding of the body, fascia, was treated as anatomically inert. It was considered wrapping. Background material. Anatomists dissected it away to reach the structures underneath.
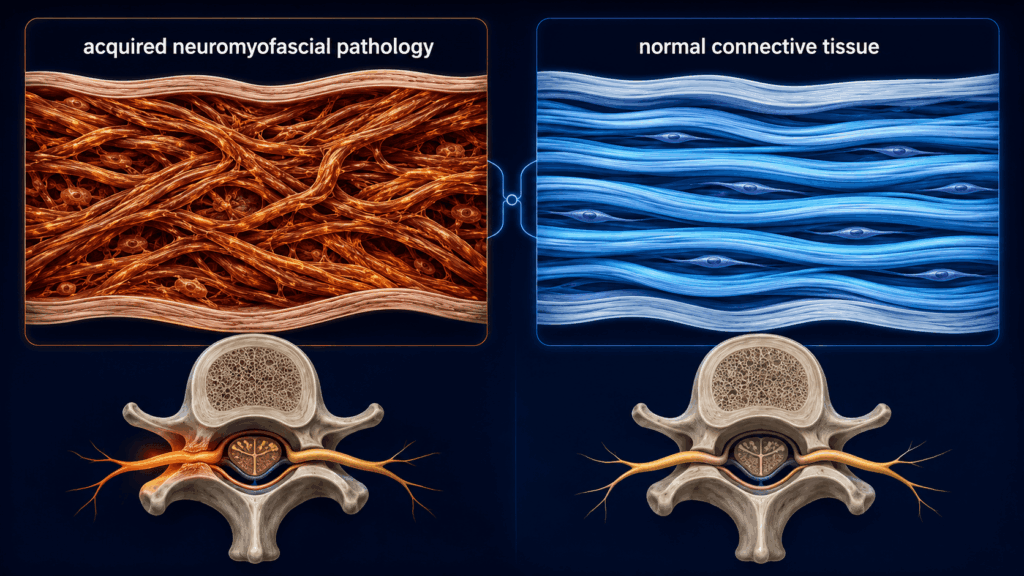
That understanding has been substantially revised. Research reviewed by Gromakovskis and colleagues (2025) supports the position that fascia is a richly innervated, biologically active tissue. It contains nociceptors, sympathetic fibers, and mechanoreceptors. It is capable of generating and transmitting pain directly. When this tissue undergoes pathological change, including densification, fibrosis, altered viscoelasticity, and impaired sliding between tissue layers, it is not a passive bystander to the pain process. It may be a primary driver of it.
This matters clinically because it changes the target. If the connective tissue itself is pathological, treating only the downstream symptom misses the source.
Measuring What Cannot Be Seen on MRI
One of the most useful recent developments in this area is the application of diagnostic ultrasound technology to connective tissue mechanics. Tomita and colleagues (2025) demonstrated measurable elevations in thoracolumbar fascia shear strain in patients with nonspecific low back pain when compared to asymptomatic individuals. Critically, these elevations correlated with patients’ pain and disability scores.
This is exactly the kind of measurement the neuromyofascial framework has been built on. The pain generators in many chronic presentations are not sitting where imaging is pointed. They are in the density, the scarring, and the altered mechanics of soft tissue. The Tomita findings confirm that those mechanics are not theoretical. They are physically present, measurable, and directly relevant to the patient’s experience.
The Spine-to-Limb Chain
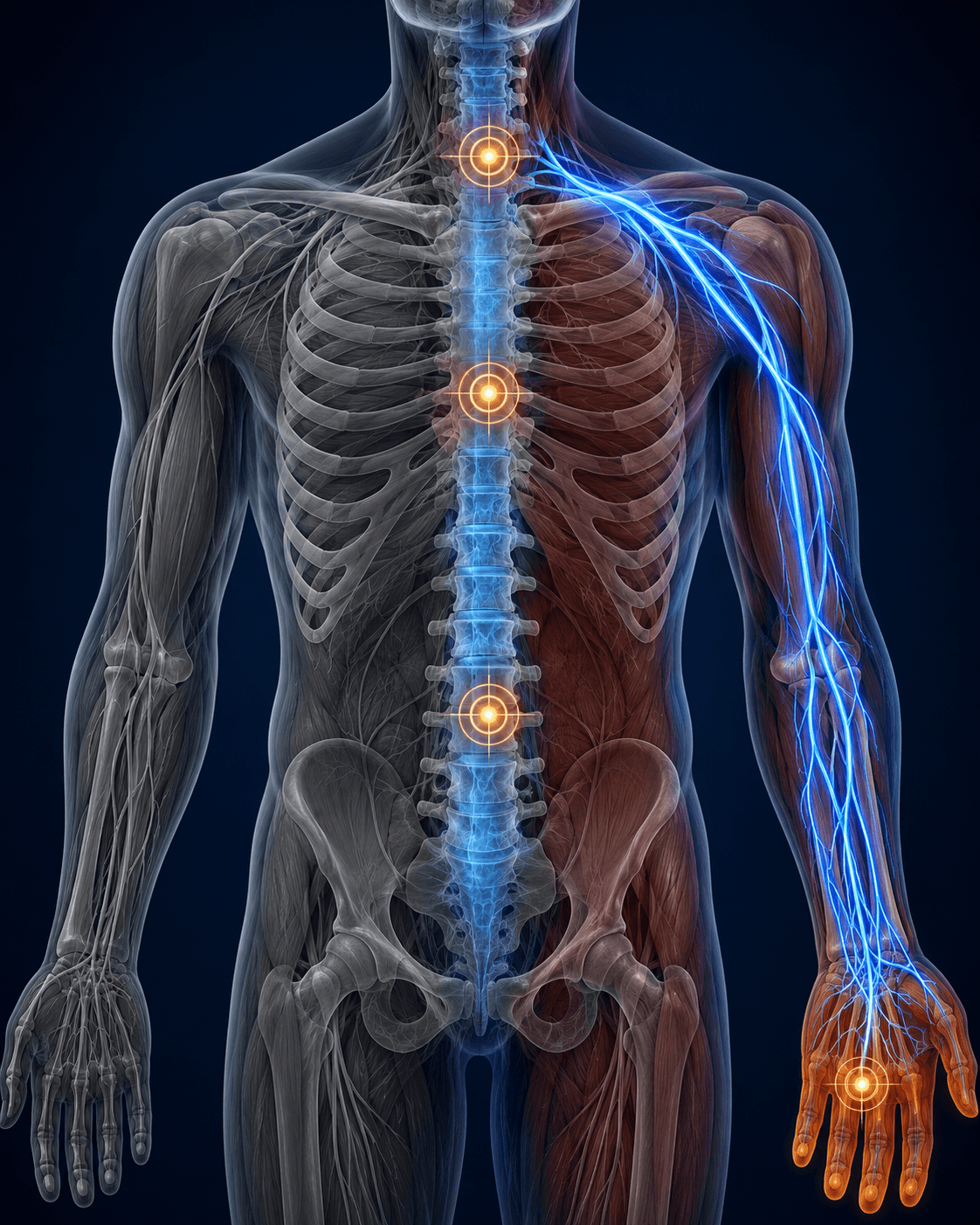
The clearest clinical demonstration of this connected architecture is what happens with carpal tunnel symptoms and hand numbness.
The intuitive assumption is that a numb hand is a wrist problem. That is where the symptoms are. That is where the standard diagnosis lands. But in the neuromyofascial framework, numbness and tingling in the hand are often downstream signals from a disruption much further up the chain. The actual site of pathology may be in the neck, at the shoulder outlet, at the axilla, or at the elbow. The wrist may be a terminal expression of a blockage that originated far above it.
The medical literature supports this logic through the concept of double crush syndrome, a recognized clinical framework in which concurrent cervical radiculopathy (nerve compression in the neck) exists alongside a peripheral nerve entrapment such as carpal tunnel syndrome in the wrist. Hansen and colleagues (2024) examined this relationship and found evidence consistent with the position that evaluating only the distal site misses a meaningful portion of the clinical picture.
The surgical data from Gullborg and colleagues (2025) makes the point even more directly. When patients underwent cervical decompression alone, treating only the neck, persistent numbness remained elevated and overall improvement in pain and disability was moderate. When surgeons addressed both the cervical spine and the peripheral nerve sites, outcomes improved substantially. Treating the whole pathway produced better results than treating one segment of it.
This is the clinical logic of the spine-to-limb chain, and it applies across far more presentations than carpal tunnel alone.
Mapping the Architecture
If the standard examination and standard imaging are not designed to locate these injury sites, a different method is required.
A specialized neuromyofascial examination is a physical process. It relies on manual evaluation of the tissue itself, identifying regions of abnormal density, restricted sliding, and altered mechanics that do not produce findings on MRI. In more advanced cases, biopsy-based auditing can confirm the exact location and nature of the pathology.
The objective of this process is not to assign a new diagnostic label. Labels are descriptions of symptoms. What the neuromyofascial audit produces is a map: precise coordinates of where the tissue is abnormal, how dense it is, and which nerves, joints, or spinal regions are being mechanically compromised as a result. That map determines the care pathway.
If the pathology is identified early, targeted self-care and tissue remodeling protocols can address the density before it compounds further. In more advanced cases, where decades of accumulation have produced significant structural burden, more intensive non-interventional or interventional approaches may be required. The map does not just identify the problem. It tells you how far it has progressed, and what level of intervention the tissue actually needs.
Why This Matters for Patients Who Have Not Found Answers
The patients who spend years carrying multiple diagnoses, cycling through specialists, and completing treatment after treatment without sustained improvement are not failing to respond. In many cases, they are being treated for the output while the input remains unaddressed.
When a stiff neck, a migraine, a numb hand, morning stiffness, and sciatica all trace back to the same underlying architecture of acquired soft tissue pathology, treating each symptom individually is an incomplete strategy. The relief, when it comes, tends to be partial and temporary. The compounding process continues because the source has not been found.
Neuromyofascial science is an attempt to answer a different question: not what label fits the symptom, but what physical site is producing it. The two embedded resources on this page, including a full explainer video and an annotated slide presentation, walk through the specific anatomy and clinical evidence in detail. The written summary above is the framework. The media below is the mechanism.
If you want to understand what is actually happening in your body, start there.
This article is written for educational purposes and represents the clinical perspective of Dr. G. Blair Lamb as developed through the neuromyofascial science framework. It is not intended as personal medical advice or as a substitute for individualized clinical evaluation. If you are experiencing chronic pain or neurological symptoms, consult a qualified healthcare provider.