Sleep disruption is one of the most commonly reported but least investigated consequences of whiplash injury. Patients describe difficulty falling asleep, frequent nighttime waking, unrefreshing sleep, and persistent daytime fatigue that does not resolve as their other whiplash symptoms improve. In many cases these symptoms are attributed to pain-related sleep disruption or to anxiety following the accident. In some cases the explanation is more structural than that.
The connection between cervical spinal injury and sleep-disordered breathing is an area of clinical observation that deserves more attention than it currently receives in standard post-whiplash care.
What the Research Shows
Several studies have examined the relationship between whiplash and sleep quality. Research led by Guilleminault identified sleep-disordered breathing as a common finding in whiplash patients, alongside daytime sleepiness, suggesting a pattern consistent with obstructive sleep apnea rather than pain-related insomnia alone. Separate work by Valenza linked the degree of sleep disturbance in whiplash patients directly to the level of ongoing pain, establishing that sleep disruption in this population is not simply a secondary psychological response but correlates with the severity of the underlying injury.
These findings point toward a physiological rather than purely psychological mechanism connecting whiplash injury to sleep quality.
The Airway Finding in James Elliott’s MRI Research
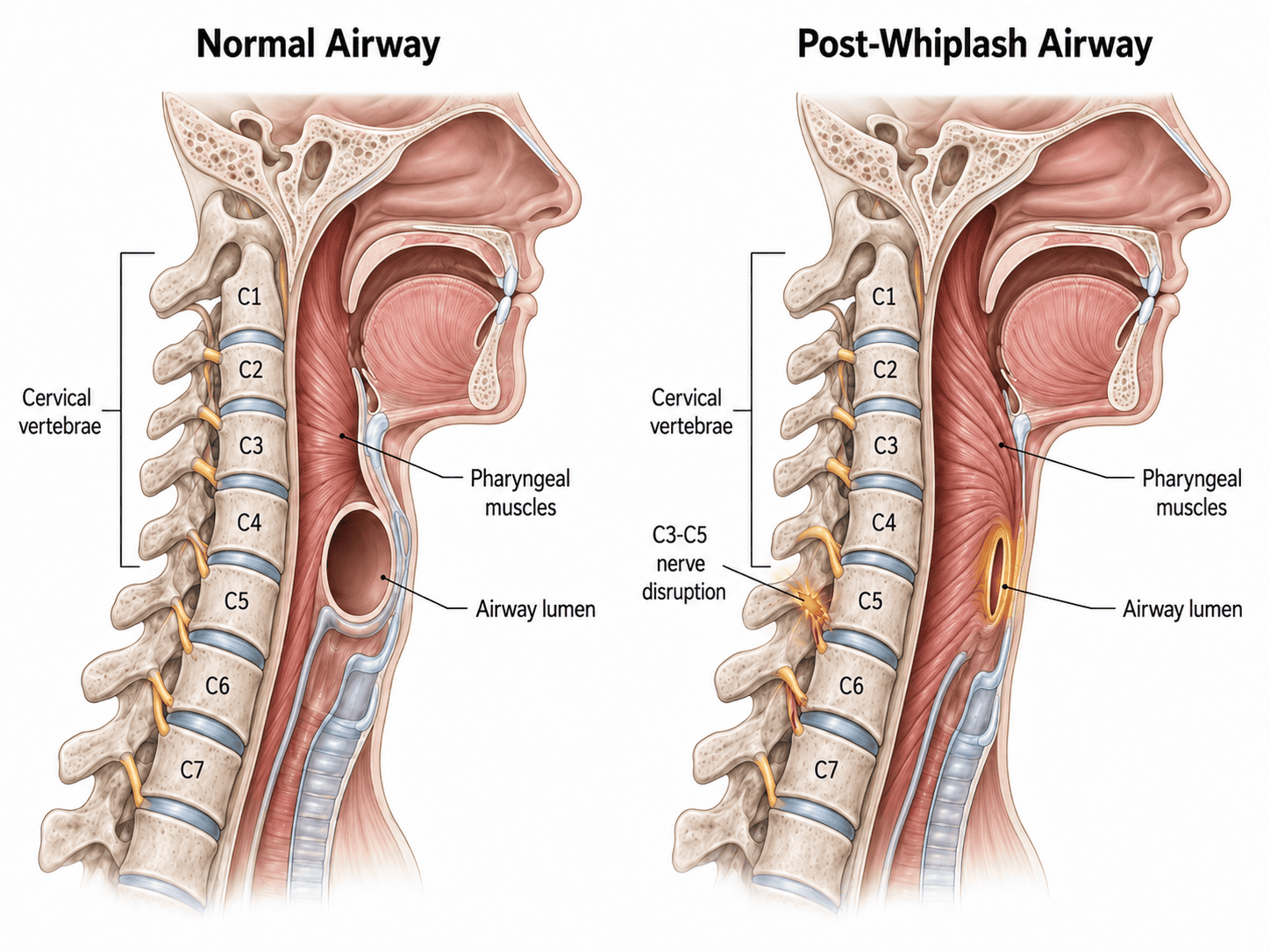
The most clinically significant piece of evidence in this area comes from the serial MRI research program led by James Elliott, whose fat water indexing work on cervical muscle injury after whiplash has been discussed elsewhere on this site. Within that same body of research, Elliott’s group identified a striking finding in severe whiplash cases: persistently altered cross-sectional airway shapes. Over time following the accident, the upper airway in these patients showed progressive narrowing and structural change in its cross-sectional geometry.
This is not a finding that standard sleep medicine or ENT workup would typically attribute to a cervical spine injury. It suggests something more specific is occurring at the level of the cervical neuromyofascial system.
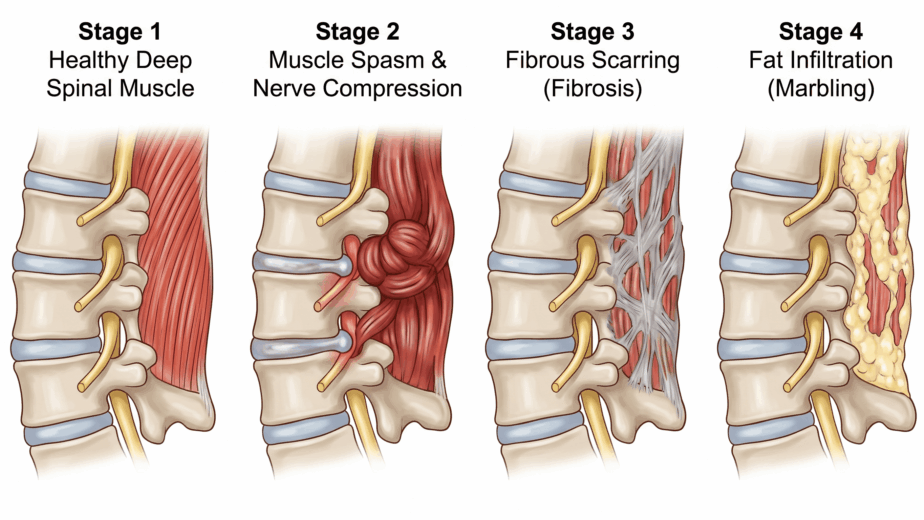
My interpretation of this finding is that it reflects whiplash-related denervation of the muscles controlling the upper airway. The cervical spine provides motor nerve supply to the smooth muscle and striated muscle of the oropharynx and upper airway. When the cervical spine sustains significant trauma, the nerve supply to these muscles can be disrupted. Denervated airway muscles behave similarly to denervated spinal muscles: they lose normal tone regulation, develop persistent spasm and shortening, and over time undergo structural change.
In the airway, this process narrows the lumen through which air passes during sleep. The result is a form of obstructive sleep apnea that originates not from obesity, anatomical variation, or central neurological causes, but from the mechanical consequences of cervical spinal injury working on the muscles of the airway.
This is a clinical hypothesis grounded in the Elliott airway finding and in the broader neuromyofascial model of cervical denervation and muscle dysfunction. It has not yet been confirmed through a dedicated clinical trial, and that research would be valuable. But it provides a mechanistically coherent explanation for why severe whiplash patients develop progressive airway changes and sleep-disordered breathing in the months following their accident.
Nighttime Urination as a Clinical Signal
One symptom pattern that I have observed consistently in whiplash patients with sleep disruption is frequent nighttime urination, specifically the sensation of needing to urinate that wakes a patient repeatedly through the night, often with only small volumes passed each time.
In conventional medicine, frequent nighttime urination prompts investigation of the bladder, prostate, kidneys, and blood sugar. Those investigations are appropriate and should be pursued. However, when those workups return normal results and the patient still reports this pattern following a whiplash event, the cervical and thoracic spine deserve consideration.
In sleep apnea, the brain generates an urge to urinate as a mechanism for waking the patient from apneic episodes, reducing the risk of prolonged oxygen deprivation. The same pattern in a whiplash patient who has not been formally diagnosed with sleep apnea may indicate that the same physiological process is occurring for the same reason: the airway is partially obstructed during sleep, the brain is generating waking signals, and the bladder urge is one of those signals.
This does not mean that every whiplash patient with nighttime urination has sleep apnea or a cervical airway problem. It means that when this symptom appears in the post-whiplash context alongside fatigue, unrefreshing sleep, and daytime sleepiness, it warrants investigation of the airway and sleep quality rather than being attributed solely to pain or anxiety.
The Broader Pattern
Sleep apnea is also more common in patients with chronic migraine, fibromyalgia, and multiple sclerosis, conditions that the neuromyofascial model associates with shared cervical and spinal injury drivers. This clustering is consistent with the NMF Science framework: when the cervical spine sustains significant injury, the downstream effects can extend across multiple systems simultaneously, including the airway and sleep architecture, in ways that are not anticipated by a symptom-by-symptom specialist model.
Patients with whiplash who are not sleeping well deserve investigation that includes the upper airway and the cervical spine, not just reassurance that pain is disrupting their rest.
The information in this article is educational and informational in nature. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. If you are experiencing sleep disturbance or other symptoms following a whiplash injury, consult with a qualified healthcare provider to discuss appropriate assessment and care.